|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
 |
||||||||||||||||||||||
|
|
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
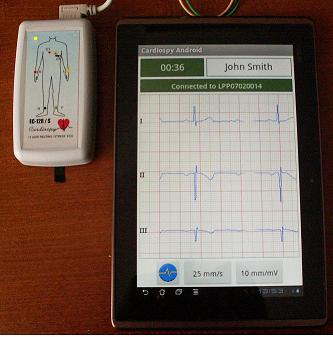
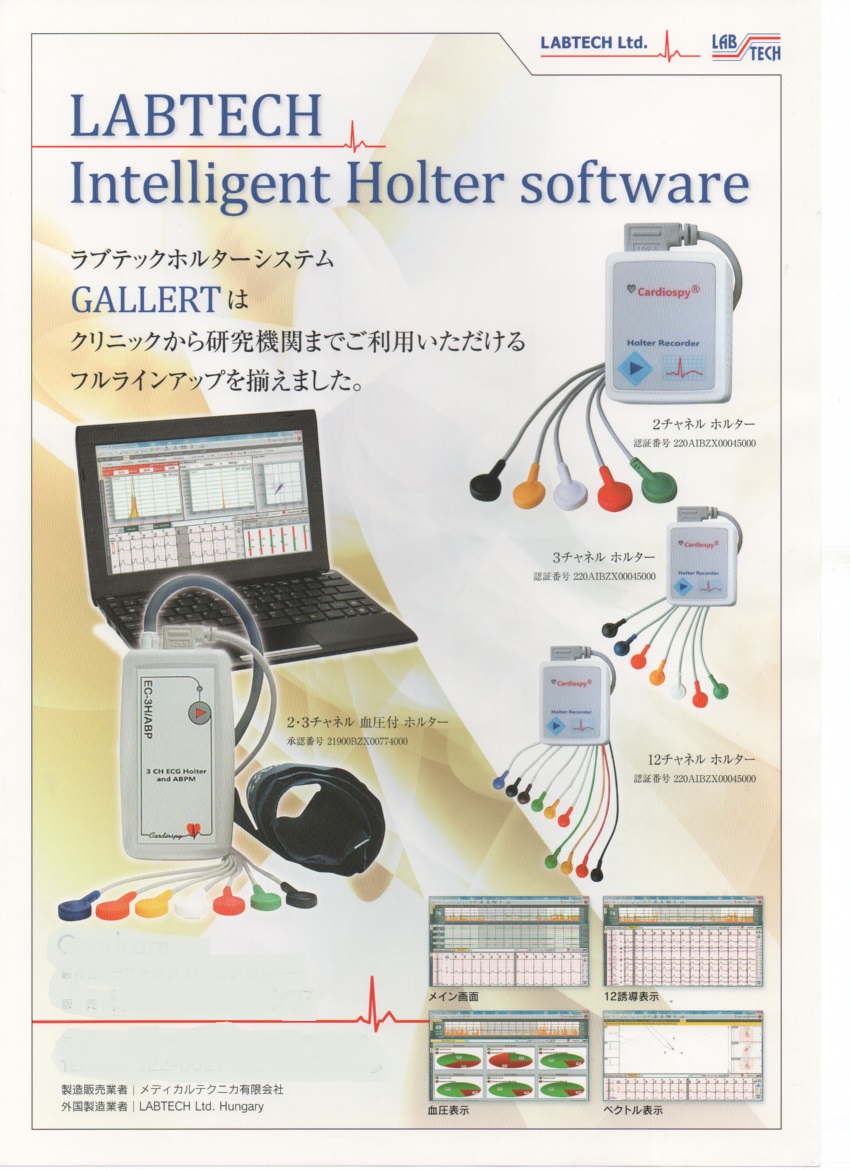
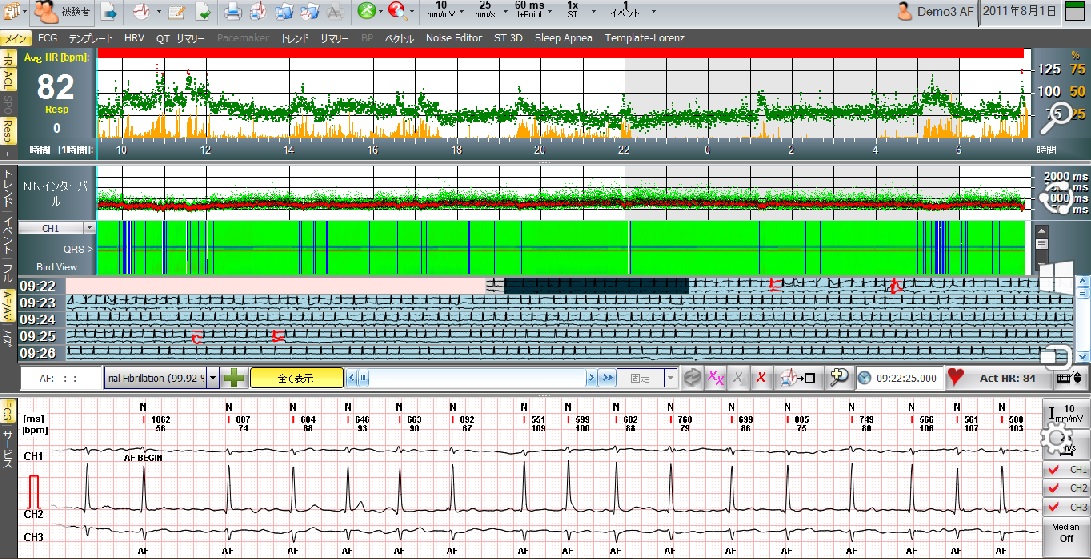
| 壓婰偼丄暰幮儔僀儞傾僢僾昳偱偡丄 | ||||||||||||||||||||||||||||
俹俠偺婡擻偑岦忋偟丄Descrete Wavelet 庤朄偑丄偍媮傔傗偡偄掅壙奿偱 幚尰偟丄怱朳偺俹攇傪帺摦専弌偱偒傞傛偆偵側傝傑偟偨丄 怱朳嵶摦偺帺摦夝愅擻傪偍帋偟帓傢傟傟偽岾偄偱偡 椪彴梡丂栻帠擣壜嵪 |
||||||||||||||||||||||||||||
Labtech幮偼丄摉幮撈帺偺曽朄偵傛傞 P攇帺摦専弌偲怱朳嵶摦帺摦夝愅庤朄偲 T Wave Alternans 夝愅庤朄傪奐敪偟丄摉幮儂儖僞乕偵搵嵹丅 |
||||||||||||||||||||||||||||
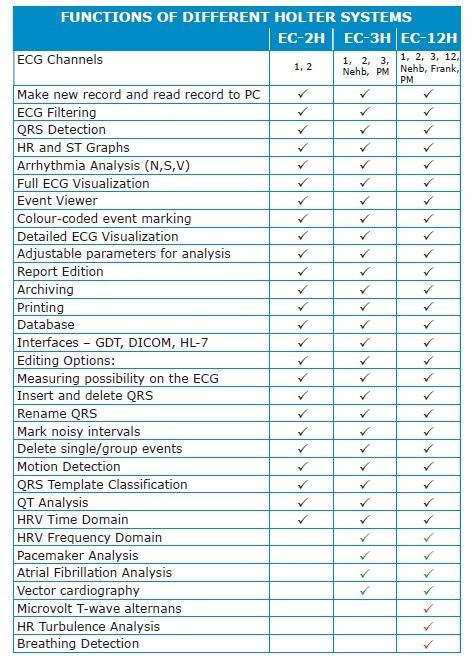
倁倕們倲倰倎俠倎倰倓倝倧倢倧倗倷,Heart Rate Variability ,TWA 僆儖僞僫儞僗 Turbulence丄俁俢壜曄昞帵丄Spectral Analysis摍偑憰旛 |
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||
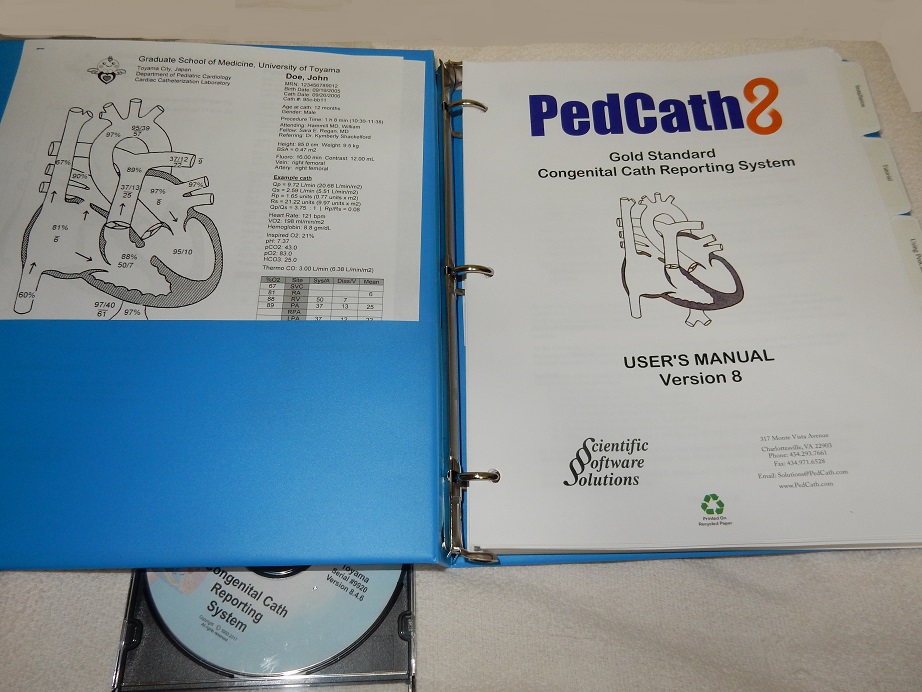
| 愭揤惈怱幘姵偺嫵壢彂丂Pedcath8 | ||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
働傾僥僀僇乕尋媶梡 旕娤寣憡懳寣埑丒楢懕丒億乕僞僽儖丒僂僄傾儔僽儖丒堦攺枅夝愅弌椡晅偒 |
||||||||||||||||||||||||||||
|
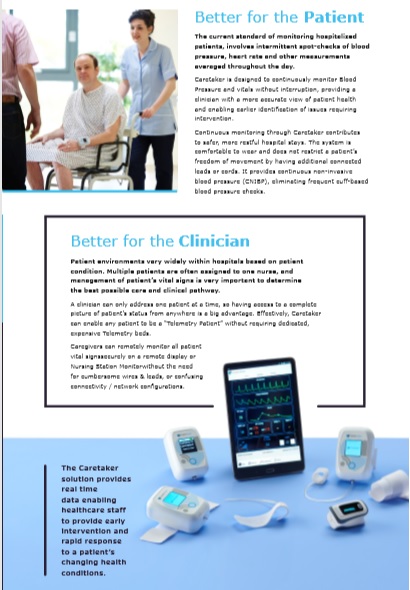
httpswww.ncbi.nlm.nih.govpmcarticlesPMC5361833 BMC Anesthesiol. 2017; 17: 48. Published online 2017 Mar 21. doi: 10.1186/s12871-017-0337-z PMCID: PMC5361833 PMID: 28327093 Continuous Non-invasive finger cuff CareTakerR comparable to invasive intra-arterial pressure in patients undergoing major intra-abdominal surgery Irwin Gratz,1 Edward Deal,1 Francis Spitz,1 Martin Baruch,2 I. Elaine Allen,3 Julia E. Seaman,4 Erin Pukenas,1 and Smith Jean1 Author information Article notes Copyright and License information Disclaimer This article has been cited by other articles in PMC. Associated Data Data Availability Statement The datasets generated during and analysed for the current study are available from the corresponding author on reasonable request. Abstract Background Despite increased interest in non-invasive arterial pressure monitoring, the majority of commercially available technologies have failed to satisfy the limits established for the validation of automatic arterial pressure monitoring by the Association for the Advancement of Medical Instrumentation (AAMI). According to the ANSI/AAMI/ISO 81060?2:2013 standards, the group-average accuracy and precision are defined as acceptable if bias is not greater than 5 mmHg and standard deviation is not greater than 8 mmHg. In this study, these standards are used to evaluate the CareTakerR (CT) device, a device measuring continuous non-invasive blood pressure via a pulse contour algorithm called Pulse Decomposition Analysis. Methods A convenience sample of 24 patients scheduled for major abdominal surgery were consented to participate in this IRB approved pilot study. Each patient was monitored with a radial arterial catheter and CT using a finger cuff applied to the contralateral thumb. Hemodynamic variables were measured and analyzed from both devices for the first thirty minutes of the surgical procedure including the induction of anesthesia. The mean arterial pressure (MAP), systolic and diastolic blood pressures continuously collected from the arterial catheter and CT were compared. Pearson correlation coefficients were calculated between arterial catheter and CT blood pressure measurements, a Bland-Altman analysis, and polar and 4Q plots were created. Results The correlation of systolic, diastolic, and mean arterial pressures were 0.92, 0.86, 0.91, respectively (p?<?0.0001 for all the comparisons). The Bland-Altman comparison yielded a bias (as measured by overall mean difference) of ?0.57, ?2.52, 1.01 mmHg for systolic, diastolic, and mean arterial pressures, respectively with a standard deviation of 7.34, 6.47, 5.33 mmHg for systolic, diastolic, and mean arterial pressures, respectively (p?<?0.001 for all comparisons). The polar plot indicates little bias between the two methods (90%/95% CI at 31.5亱/52亱, respectively, overall bias?=?1.5亱) with only a small percentage of points outside these lines. The 4Q plot indicates good concordance and no bias between the methods. Conclusions In this study, blood pressure measured using the non-invasive CT device was shown to correlate well with the arterial catheter measurements. Larger studies are needed to confirm these results in more varied settings. Most patients exhibited very good agreement between methods. Results were well within the limits established for the validation of automatic arterial pressure monitoring by the AAMI. Keywords: Non-Invasive, CareTaker, Central blood pressure, Finger cuff, Intra-Arterial pressure |
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|