|
|
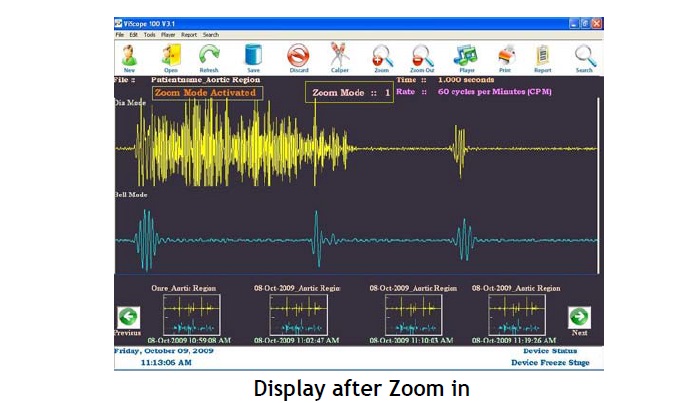
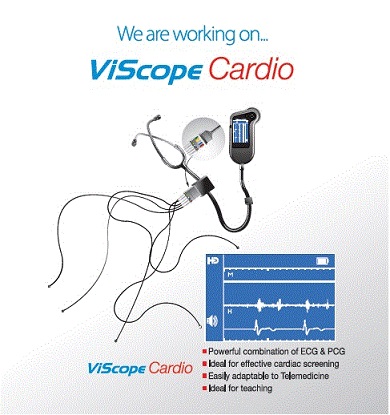
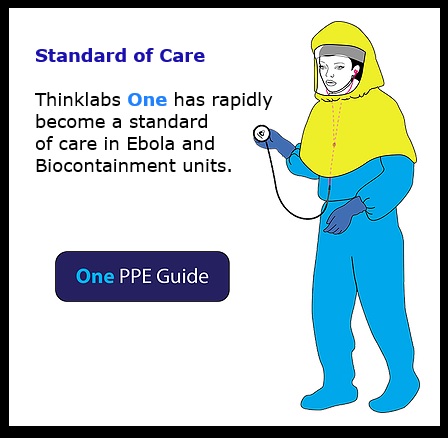
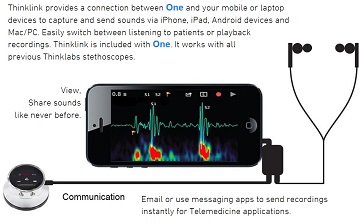
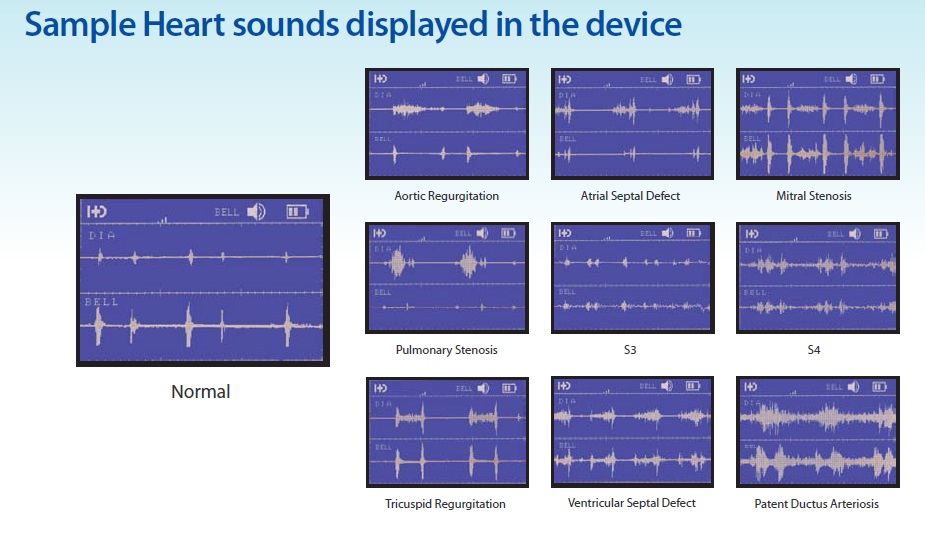
#電子聴診器 #HDmedical社が
#画面付き、且つ、#聴診音解析する #電子聴診器
(薬事未認可に付き注意)
|
|
|
|
|
|
|
|
|
|
#VitalStream
#メディカルテクニカが、#2007年から #研究用にご案内して参りました
#非観血で、#連続観血血圧を解析できる #世界初の血圧計は、
#最新ディジタル機能を搭載して#名称変更しご案内申し上げます
#VitalStream #バイタルストリーム
タイプ1、タイプ2、タイプ3と当面分かれています、
タイプ1は、以前の #Caretaker_type5の名称変更です、
従来品は、#Caretaker_type1_type2_type3_type4でした
日々仕様が改良され、最先端のセンサー採用・解析項目の多様化
最先端ディジタルの取り込み等が必ずお問い合わせ願います、
メディカルテクニカでは #バックアップをご用意しております
|
|
|
|
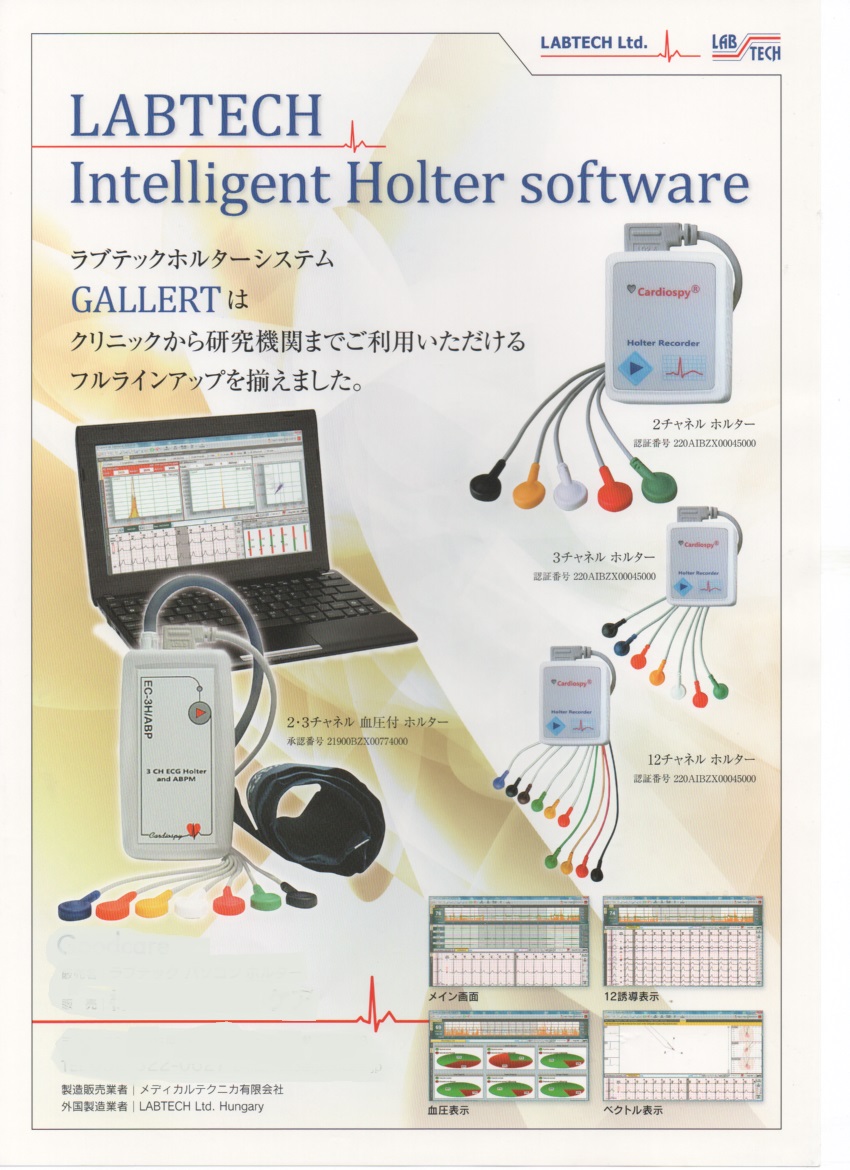
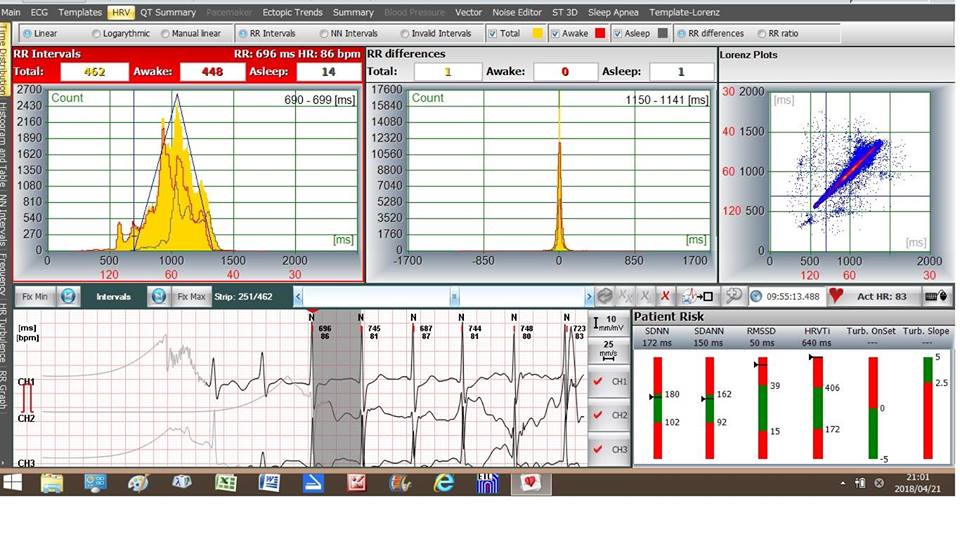
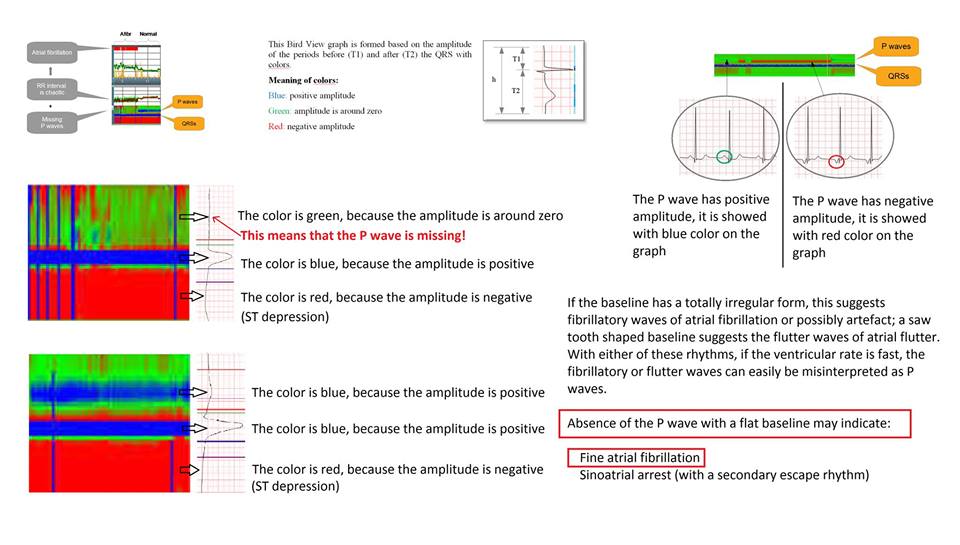
#Labtech_Hungary #wireless_12leads_ECG_Holter
#メディカルテクニカが #2002年本邦に導入し、
#薬事承認は2008年取得し、数回設計変更で対応
#救急車にご採用の #モバイル12誘導心電計はこの #Labtech社です、
#メハーゲン社が大半の株主で日本市場に安心をご提供しております、
最近、#心疾患の正しい診断方法として、本来 #心臓が電気信号で動いている
事から、#心臓自身の電気信号診断として脚光を受けるようになりました、
特に、#ベクトル心電図は、#連続的に、#wavelet_algorithm により、
ノイズはディジタル式に除去され、また、解析もディジタル化され、
素晴らしいデータをご提供します、
本ディジタル化は、#負荷心電図で既に国内にかなりご採用頂いております、
|
|
|
|
 |
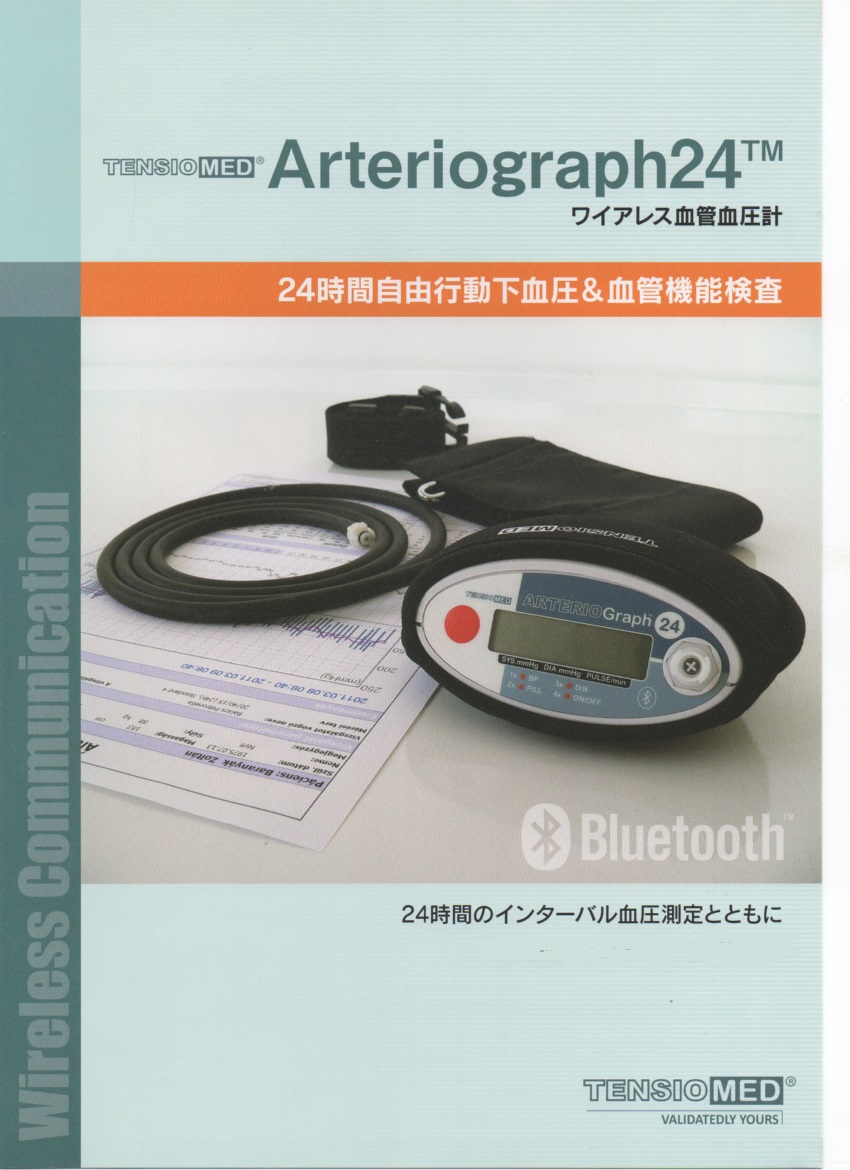
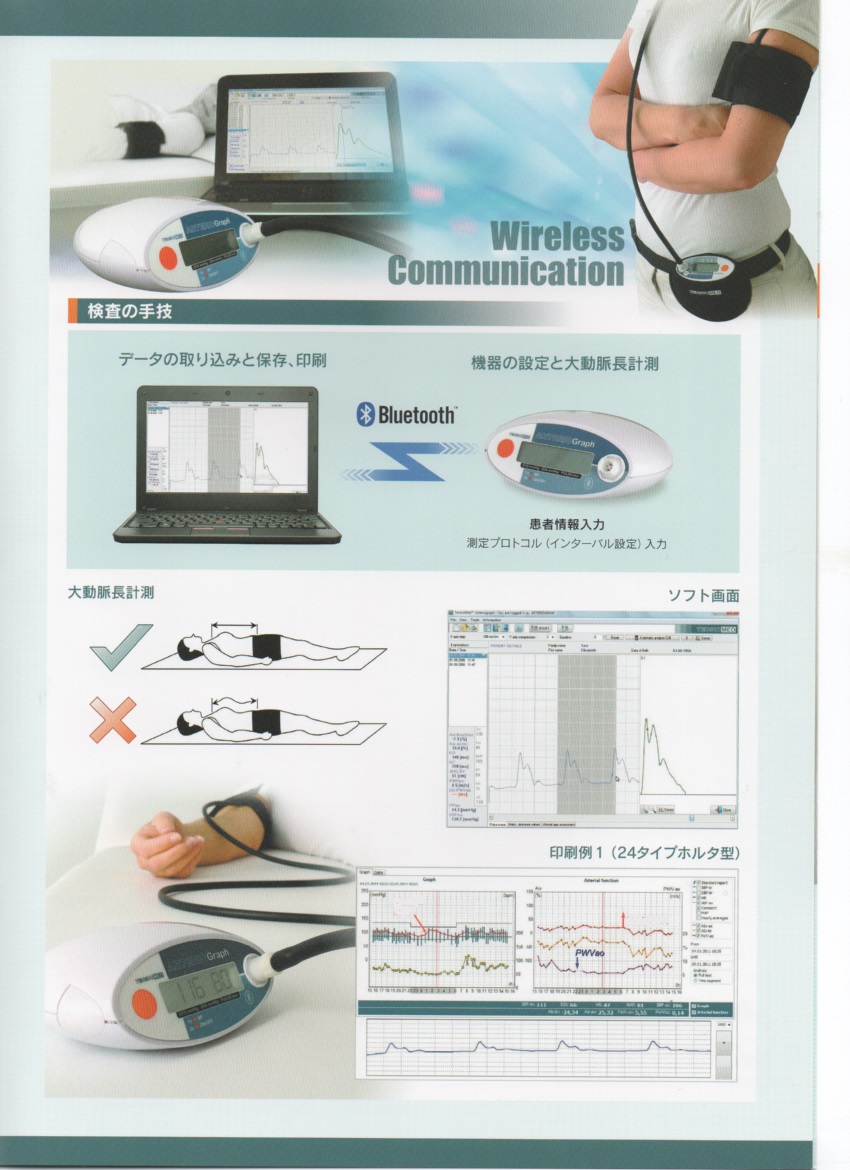
(#Arteriograph) #Arteriograph24
#診療報酬有
#動脈硬化指標を24時間から72時間トレンド計測 #三分間で測定
欧州米国特許有 日本特許有 携帯電話及びインターネット利用、
高脂血症、高血圧、肥満、生活習慣病、腎臓病、内分泌などが原因か
#ドイツ最大製薬会社の#指定機器
で #世界でご採用になっています
|
|
|
|