|
Central blood pressure: current evidence
and clinical importance
Carmel M. McEniery1*, John R. Cockcroft2, Mary J. Roman3, Stanley S. Franklin4, and Ian B.Wilkinson1
1Clinical Pharmacology Unit,
University of Cambridge, Addenbrooke’s Hospital, Box 110, Cambridge CB22QQ, UK;
2Department of Cardiology,Wales Heart Research Institute, Cardiff
CF14 4XN, UK; 3Division of Cardiology,Weill Cornell Medical College, New York, NY
10021, USA; and 4University of California, UCI School of Medicine, Irvine, CA
92697-4101, USA Received 29 April 2013;
revised 27 November 2013; accepted 17 December 2013; online
publish-ahead-of-print 23 January 2014
and central pressure. Therefore, basing treatment decisions on
central, rather than brachial pressure, is likely to have important
implications
for the future diagnosis and management of hypertension. Such a
paradigm shift will, however, require further, direct evidence that selectively
targeting central pressure, brings added benefit, over and above
that already provided by brachial artery pressure. Keywords Central pressure †
Blood pressure †
Anti-hypertensive treatment †
Cardiovascular risk
Introduction
The brachial cuff sphygmomanometer was introduced into medical practice well over 100 years ago, enabling the routine,
non-invasive,
measurement of arterial blood pressure. Life insurance companies were among the first to capitalize on the information provided by
cuff sphygmomanometry, by observing that blood pressure in largely asymptomatic individuals relates to future cardiovascular
risk—observations that are nowsupported by a wealth of
epidemiological data.1 The most recent Global Burden of Disease report2
identified hypertension as the leading cause of death and
disability worldwide. Moreover, data from over 50 years of randomized
controlled
trials clearly demonstrate that lowering brachial pressure, in hypertensive individuals, substantially reduces cardiovascular
events.1,3 For these reasons, measurement of brachial blood pressure has become embedded in routine clinical assessment throughout the
developed world, and is one of the most widely accepted ‘surrogate measures’ for regulatory bodies.
The major driving force for the continued use of brachial blood pressure has been its ease of measurement, and the wide variety of
devices available for clinical use. However, we have known for
over half a century that brachial pressure is a poor surrogate for
aortic
pressure, which is invariably lower than corresponding brachial values. Recent evidence suggests that central pressure is also
more
strongly related to future cardiovascular events4 – 7 than brachial pressure, and responds differently to certain drugs.8,9 Appreciating
this provides an ideal framework for understanding the much
publicized inferiority of atenolol and some other beta-blockers,10 compared
with other drug classes, in the management of essential hypertension. Although central pressure can now be assessed
noninvasively
with the same ease as brachial pressure, clinicians are unlikely to discard the brachial cuff sphygmomanometer without
robust evidence that cardiovascular risk stratification, and
monitoring response to therapy, are better when based on central rather
than peripheral pressure. Central pressure assessment and accuracy will also have to be standardized, as it has been for brachial
pressure
assessment with oscillometric devices. This review will discuss
our current understanding about central pressure and the evidence
required to bring blood pressure measurement, and cardiovascular risk assessment into the modern era. Physiological concepts Arterial pressure varies continuously over the cardiac cycle, but
in
clinical practice only systolic and diastolic pressures are
routinely reported. These are invariably measured in the brachial artery using cuff sphygmomanometry—a practice that has changed little
over the last century. However, the shape of the pressure waveform * Corresponding author. Tel: +44 1223 336806, Fax: +44 1223 216893, Email: cmm41@cam.ac.uk
Published on behalf of the European Society of Cardiology. All
rights reserved. &The Author 2014. For permissions please email:
journals.permissions@oup.com European Heart Journal (2014) 35, 1719–1725 doi:10.1093/eurheartj/eht565
Pressure measured with a cuff and sphygmomanometer in the brachial
artery is accepted as an important predictor of future cardiovascular
risk.However, systolic pressure varies throughout the arterial tree, such that
aortic (central) systolic pressure is actually lower than corresponding brachial values, although this difference is
highly variable between individuals. Emerging evidence now suggests that
central pressure is better related to future
cardiovascular events than is brachial pressure. Moreover, anti-hypertensive
drugs can exert differential effects on brachial and
central pressure. Therefore, basing treatment decisions on central, rather than
brachial pressure, is likely to have important implications for the future diagnosis and management of hypertension. Such a
paradigm shift will, however, require further, direct evidence that selectively targeting central pressure, brings added benefit, over and above
that already provided by brachial artery pressure.As discussed earlier, a full
synthesis of the available evidence concerning
central pressure and the risk of future cardiovascular events is now required. However, it will also be necessary
to determine the clinical relevance of differences
between brachial and central pressurefor the individual patient, especially given the relatively high
correlation between the
two. Emerging data support the prognostic superiority
of both 24-h ambulatory blood pressure monitoring(ABPM)79 – 81 andhomemonitoring81 in comparison with office measurements. Interestingly, a recent study82 demonstrated that 24-h ambulatory cuff pressures were comparable with
office central pressuremeasurements in the prediction of risk, although the significance of this study awaits confirmation.83 As yet, there are no data
comparing the
predictive value ofhomemonitoring vs. central pressure in theprediction of risk. Ultimately, it will be necessary to evaluate
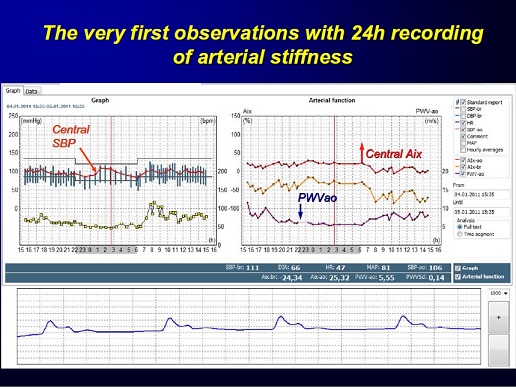
the prognostic value of 24-h
ambulatory central pressure.With the recent development of ambulatory central pressure systems,84,85 this is nowpossible and it may be reasonable to hypothesize that 24-h
central, rather than
brachial ABPM would be superior in terms of risk prediction.
|