|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
ViScope100 聴診音が、その計測部のダイヤフラムの部分に連続表示されます。 また、SDカードに記憶されたデータは専用ソフトウエアでパソコンに表示記憶できます。 |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
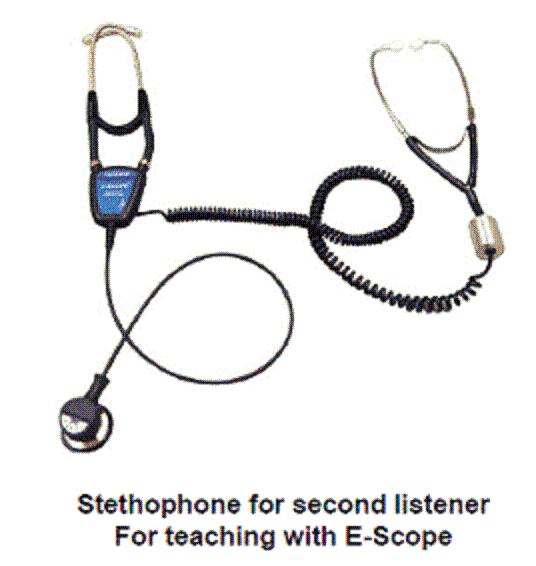
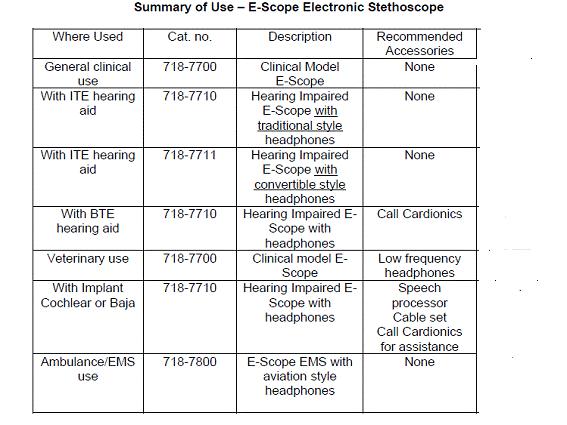
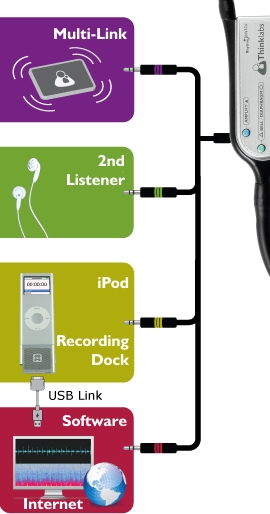
1. 聴診音の教育用として、 電子ヘッドホンを多数の生徒が同時に聞くことができる。 電波距離約10mで、電子聴診器部で送信ボタンを押す 2.iPhone でも聴診音を受信・音声聴診できる 3.電子カルテなどのソフトウエアへ送信できる 4.ペットの処置等に、ペットの心音をモニターできる 5.標準二分間稼動するが、一時間まで設定を変えることができる 6.耳が不自由な医療従事者に、有効なツールとして採用頂く 7.歯科医師等の歯科処置中に、患者の心音又は呼吸音をモニターできる 8.危険物・有害物を扱う場面での有効なモニター方法を提供する 9.救命救急時の、救急車中などの用途として役立つ. 10、スポーツ、リハビリ、在宅看護、山間部、 離島などの遠隔監視用として有効 |
||||||||||||||||||||||
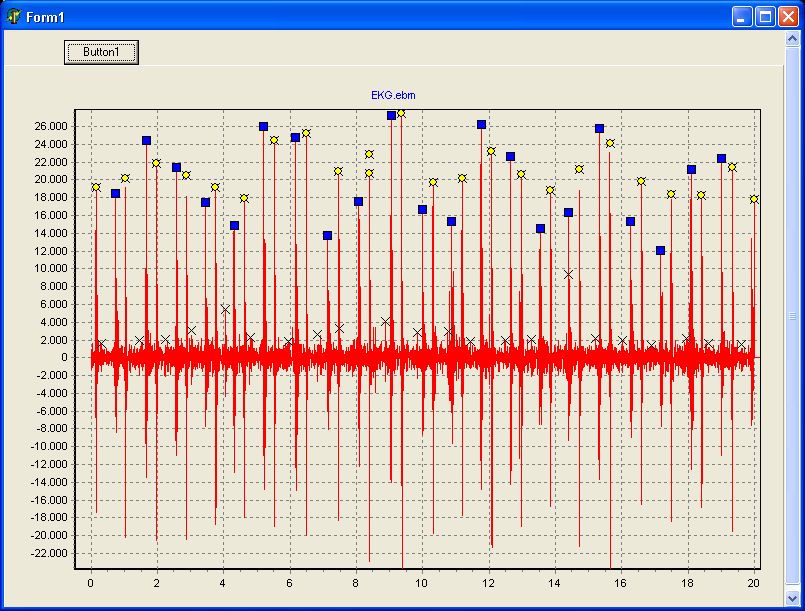
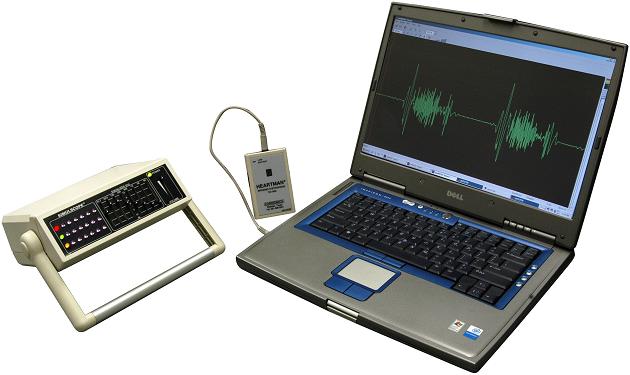
iPod, iPad, iPhone 等による 聴診音の リアルタイム 連続波 表示、記憶、記録、他へ転送、が安い価格で可能となりました。 、 |
||||||||||||||||||||||
当カルディオニクス社製シミュレータについては、 概要を下記にてご案内しております。 各種シミュレータはこちら 販売を希望される会社を募集 |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
iPod, iPad, iPhone 等に、画像化表示するシステムをご案内します。 其の他、お問い合わせ下さい。
http://www.din.or.jp/~meditekn/medi_hp/ |
||||||||||||||||||||||
|
||||||||||||||||||||||
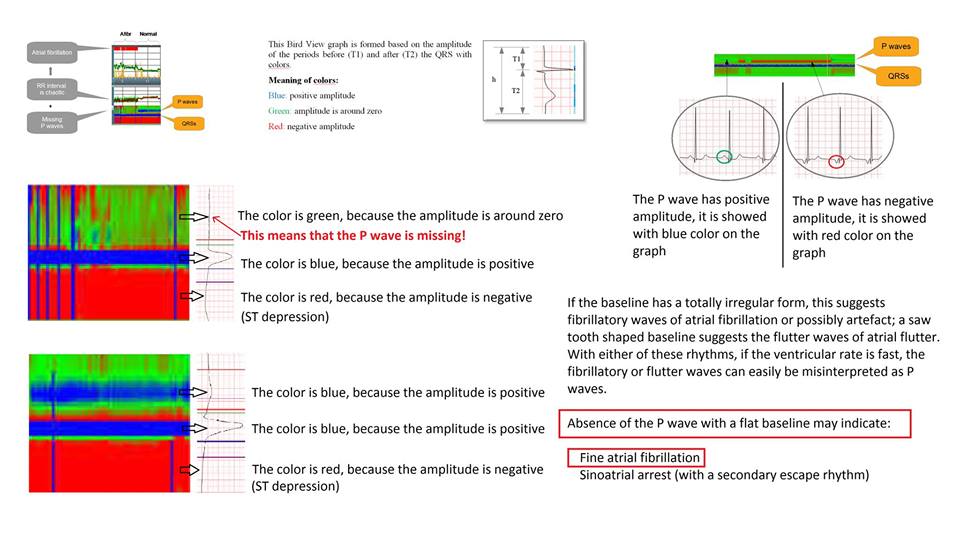
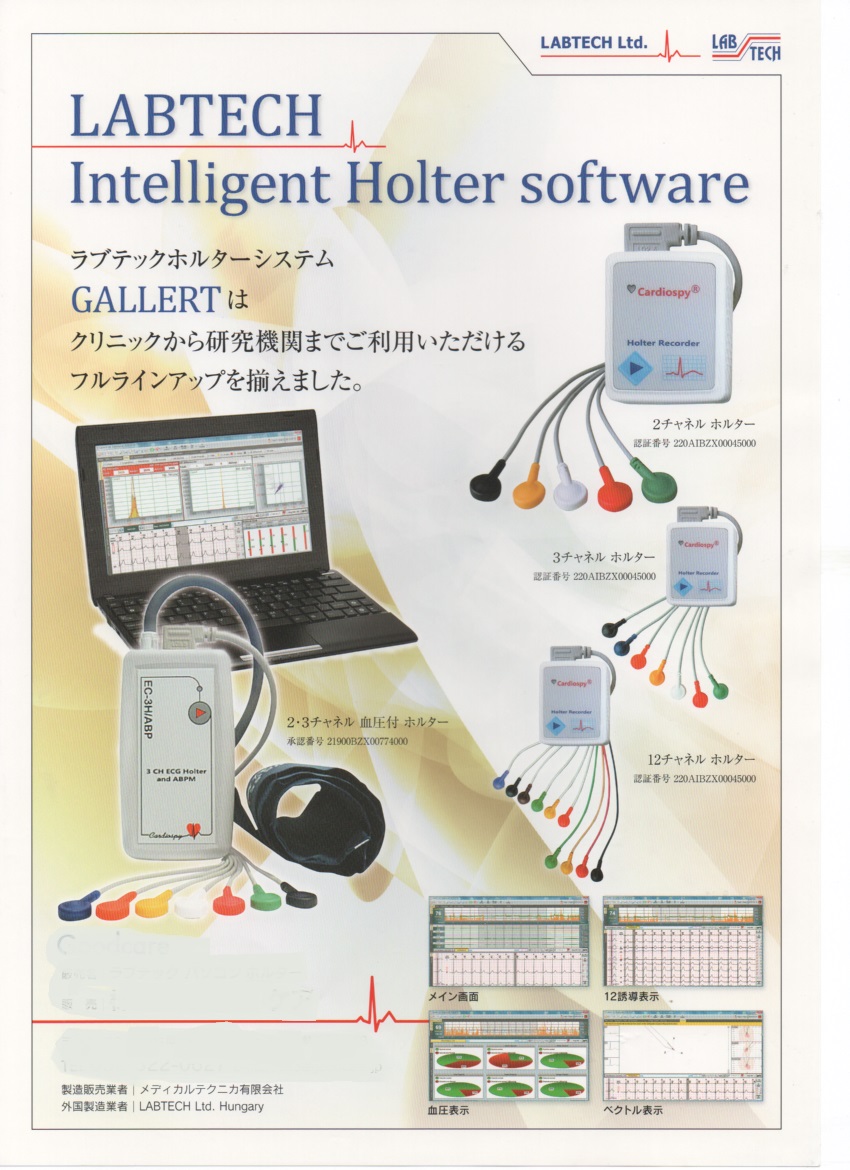
世界初、周波数分析の一種の wavelet 新技術で、12誘導心電図を、 基線安定・ノイズ除去・周波数解析 完全ディジタル化ーネット化・スマホ化・科学演算などを可能しています、 本原理は、1900年初めに、Hungary 生まれ、Alfred Haar の発明です、 医療循環器分野で有名な応用は、レートポテンシャル・P波検出・モニターがありました 今回ハンガリ国ラブテック社により、 スマホモバイル12誘導心電計・パソコン式12誘導負荷心電計 そして P波自動検出ホルター心電計・連続解析ベクトルホルター心電計です、 又、静止心電図はもちろん上記心電図等の一括さ^バー記憶呼出が可能です、 未だ文献の無い12誘導心電計出力にQRS波形の同時8チャンネル出力が放置されています |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
 |
||||||||||||||||||||||
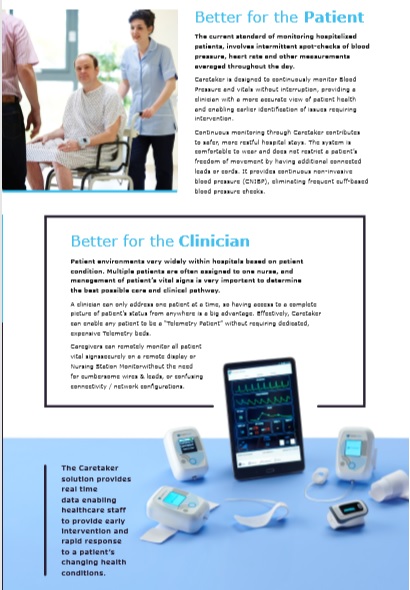
#VitalStream #バイタルストリーム #非観血式で、#観血血圧を連続解析する #生体情報モニター #世界初 #2017年米国FDAに承認 #解析項目_血行動態20種類 プラス #特定センサー情報を同時表示・ご利用項目演算可能 モデル タイプ1,タイプ2,タイプ3 (タイプ1は、#Caretaker_type4 の改名) 特徴 #世界最先端ディジタル技術搭載、#ワイヤレスはbluetooth_WiFi,選択 #SDKオプション #人工知能ソフト無料参加、#Tabletにスマホ追加可、#Net技術ご利用可、 #他社センサー類機能追加可、#最新人工知能ソフト追加可、 詳細お問い合わせは #メディカルテクニカ (#2007年から導入)へ |
||||||||||||||||||||||
|