|
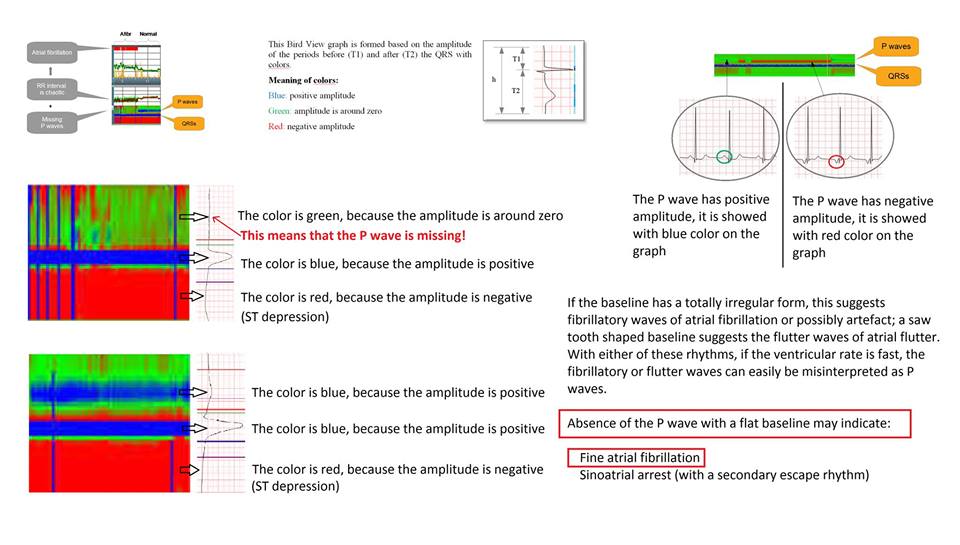
Theory of the #P_wave_detection
The algorithm first
finds the the possible positive and
negative wave peaks based on zero transition searching, then validates them
with comparing to reference P waves.
The P wave detection
needs high amplitude resolution. This value is better, than 0.6 uV / bit in the
Cardiospy system. With this resolution
and the effective filter system which uses wavelet transformation, the Cardiospy
system is able to detect P waves less than 50 uV of amplitude.
Validation of the #P_wave_detector
The validation is
carried out on 10 pcs 12 channel and 10 pcs 3 channel ECG reference records.
The reference records include the P wave
annotation. 12 of the 20 records
are taken from the MitBih database, 8 records are taken from the Labtech
database (30000 – 30007).
12 ch records
s0014lre, s0292lre,
s0302lre, s0331lre, s0364lre, s0422_re, s0431_re, s0437_re, s0549_re, s0550_re
3 ch records
mgh001, mgh007,
30000, 30001, 30002, 30003, 30004, 30005, 30006, 30007
Validation result:
Sensitivity: 95.42%
Positive
predictivity: 97.16%
|