中心血圧機能の検証---不思議?ドイツ最大の製薬会社が2015年から世界の標準器で利用
#動脈硬化、#高血圧、#冠動脈疾患、#大動脈疾患、#透析、#血管老化度などで
重要なパラメータの #PWVao,#AIX,などを算出します。
ワイヤレス、コードレス、携帯式で、軽く、取り扱い便利で、場所を取りません。
ホルタ式で、一日などの経過を計測できます。
|
|
#Central_blood_pressure: current evidence and clinical importance
Carmel M. McEniery1*, John R. Cockcroft2, Mary J. Roman3,
Stanley S. Franklin4, and Ian B.Wilkinson1
1Clinical
Pharmacology Unit, University of Cambridge, Addenbrooke’s
Hospital, Box 110, Cambridge CB22QQ, UK; 2Department of Cardiology,Wales Heart Research Institute,
Cardiff
CF14 4XN, UK; 3Division
of Cardiology,Weill Cornell Medical College, New York, NY 10021, USA; and 4University of California, UCI School of
Medicine, Irvine, CA 92697-4101, USA
Received 29 April 2013;
revised 27 November 2013; accepted 17 December 2013; online
publish-ahead-of-print 23 January 2014
and central pressure. Therefore, basing treatment decisions on central,
rather than brachial pressure, is likely to have important implications
for the future diagnosis and management of hypertension. Such a paradigm
shift will, however, require further, direct evidence that selectively
targeting central pressure, brings added benefit, over and above that
already provided by brachial artery pressure.
Central pressure † Blood pressure † Anti-hypertensive treatment † Cardiovascular risk
Introduction
The brachial cuff sphygmomanometer was introduced into medicalpractice
well over 100 years ago, enabling the routine, non-invasive,
measurement of arterial blood pressure. Life insurance companieswere among
the first to capitalize on the information provided by
cuff sphygmomanometry, by observing that blood pressure inlargely asymptomatic
individuals relates to future cardiovascular
risk—observations that are nowsupported by a wealth of
epidemiologicaldata.1 The most recent Global Burden
of Disease report2
identified hypertension as the leading cause of death and disabilityworldwide.
Moreover, data from over 50 years of randomized controlled
trials clearly demonstrate that lowering brachial pressure,in hypertensive
individuals, substantially reduces cardiovascular
events.1,3 For these reasons, measurement of brachial blood pressurehas become embedded in routine clinical assessment throughout
thedeveloped world, and is one of the most widely accepted ‘surrogatemeasures’ for regulatory bodies.
The major driving force for the continued use of brachial bloodpressure
has been its ease of measurement, and the wide variety of
devices available for clinical use. However, we have known for overhalf
a century that brachial pressure is a poor surrogate for aortic
pressure, which is invariably lower than corresponding brachialvalues.
Recent evidence suggests that central pressure is also more
strongly related to future cardiovascular events4 – 7 than brachialpressure, and responds differently to certain drugs.8,9 Appreciating
this provides an ideal framework for understanding the much publicizedinferiority
of atenolol and some other beta-blockers,10 compared
with other drug classes, in the management of essentialhypertension. Although
central pressure can now be assessed noninvasively
with the same ease as brachial pressure, clinicians are unlikelyto discard
the brachial cuff sphygmomanometer without
robust evidence that cardiovascular risk stratification, and monitoringresponse
to therapy, are better when based on central rather
than peripheral pressure. Central pressure assessment and accuracywill
also have to be standardized, as it has been for brachial pressure
assessment with oscillometric devices. This review will discuss ourcurrent
understanding about #central_pressure and the evidence
required to bring #blood_pressure_measurement, and #cardiovascularrisk_assessment
into the modern era.
#Physiological_concepts
Arterial pressure varies continuously over the cardiac cycle, but inclinical
practice only systolic and diastolic pressures are routinely
reported. These are invariably measured in the brachial arteryusing cuff
sphygmomanometry—a practice that has changed
little
over the last century. However, the shape of the pressure waveform* Corresponding
author. Tel: +44 1223 336806, Fax: +44 1223 216893, Email: cmm41@cam.ac.uk
Published on behalf of the European Society of Cardiology. All rights
reserved. &The Author 2014. For
permissions please email: journals.permissions@oup.com
European Heart Journal (2014) 35, 1719–1725 doi:10.1093/eurheartj/eht565
Pressure measured with a cuff and sphygmomanometer in the brachial artery
is accepted as an important predictor of future cardiovascular risk.
However, systolic pressure varies throughout the arterial tree, such that
aortic (central) systolic pressure is actually lower than corresponding
brachial values, although
this difference is highly variable between individuals. Emerging evidence now
suggests that central pressure is better
related to
future cardiovascular events than is brachial pressure. Moreover, anti-hypertensive
drugs can exert differential effects on brachial
and
central pressure. Therefore, basing treatment decisions on central, rather than
brachial pressure, is likely to have important implications
for the future diagnosis and management of hypertension. Such a
paradigm shift will, however, require further, direct evidence that selectively
targeting central pressure, brings added benefit, over and above that already
provided by brachial artery pressure.As discussed earlier,
a full synthesis of the available evidence concerning
central pressure and the risk of future cardiovascular events is now required. However, it will also be necessary to determine
the clinical
relevance of differences between brachial and central pressurefor the individual patient, especially given
the relatively high correlation between the two. Emerging data support the prognostic superiority of both 24-h ambulatory blood pressure monitoring
(ABPM)79 – 81 andhomemonitoring81 in comparison with office measurements. Interestingly, a recent
study82 demonstrated that
24-h ambulatory cuff pressures
were comparable with office central pressure
measurements in the prediction of risk, although the significance of this study awaits
confirmation.83 As yet,
there are no data comparing
the predictive value ofhomemonitoring vs. central
pressure in theprediction of risk. Ultimately, it will be necessary to evaluate
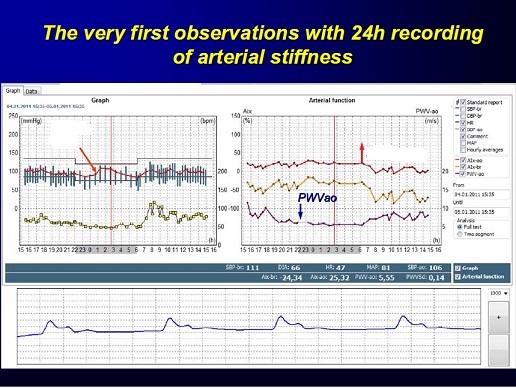
the prognostic value of 24-h ambulatory central pressure.With the recent
development of ambulatory central pressure systems,84,85 this is now
possible and it may be reasonable to hypothesize that 24-h central, rather than brachial ABPM
would be superior in terms of risk prediction.
|
測定パラメータ一覧 (ご注意、各機種により、測定項目が異なります)
#収縮期圧、#拡張期圧、#大動脈収縮期圧、#大動脈脈圧、検証募集中の#平均動脈圧、#脈圧、#心拍数、
、
ブルーツース式24時間又は72時間携帯式血圧記録 (統計演算各値付き)
#Arteriograph ,#SBP,#DBP,#MAP,#PP,#HRT,#AugumentationIndex,など
#日本_米国等の特許取得済み
欧州を中心に米国・中近東・アジア諸国でご採用、
|
|
|
|
|
| American Journal of Hypertension ajh.oxfordjournals.org
Am J Hypertens (2005) 18 (S4): 15A. doi:
10.1016/j.amjhyper.2005.03.035 P-17: A new
and fast screening method for measuring complex
hemodynamical parameters and arterial stiffness
non-invasively with a simple arm cuff Miklos
Illyes1 + Author Affiliations 1TensioMed
Ltd., TensioMed Ltd, Budapest, Hungary Abstract
Aims: In a project of the National Research
Program of Hungary, we studied if oscillometric
signals received during an oscillometric
BP measurement contain any information about
arterial hemodynamics Materials, Methods:
We have developed a research tool by which
not only SBP, DBP, HR data, but the complete
oscillometric signals were stored and transmitted
telemedically to our computer center from
the home of 650 patients who performed BP
measurements at least 4 times a day, for
at least 1 month. Through this a large database
was collected, containing more than 1700000
oscillometric pulse curves and the relevant
clinical data of patients. For data mining
we used Kohonen's self-organising map method.
Non-invasively recorded oscillometric curves
from the upper arm cuff were validated by
the simultaneously recorded intraarterial
pressure curve of brachial artery. Results:
Our researches showed that oscillometric
pulse curve of the brachial artery is identical
to the intraarterial pressure curve if the
cuff was inflated to suprasystolic pressure,
preferably 35 mmHg above the SBP. Thus the
early and the late systolic pressure peak,
the closing incisure of the aortic valve
can be recognizable, and several hemodinamical
parameters could be calculated. By using
the mentioned results of basic researches,
a new instrument, the TensioClinic Arteriograph
was developed, by which the following parameters
could be measured within 2 minutes, by using
a simple upper arm cuff: SBP, DBP, HR, MAP,
PP, augmentation index (AIx), normalized
augmentation index to 80/min heart rate (AIx80),
return time of the pulse wave of the aorta
(RT), pulse wave velocity (PWV) of the aorta,
length of the cardiac cycle, area of systolic
(SAI) and diastolic (DAI) part of pulse curve.
Validation studies of the new method to control
the accuracy of measured AIx and PWV showed
high correlations (R = 0,76 and R = 0,8)
with values measured with other non-invasive
methods (Sphygmocor and Complior) respectively.
Conclusions: Due to the swiftness, simplicity
and good reproducibility of this method and
apparatus, the non-invasive assessment of
the most important hemodynamical parameters
and arterial stiffness had become available
for population screening, opening a new window
in the detection of the early phase of the
athero- and arteriosclerosis, and thus it
can play an important role in the reduction
of the CV morbidity and mortality. |
|
| ドイツ 医学 科学誌掲載 2005年
oszillometrisch mit Arteriograph (TensioMed,
Budapest) " " J. Baulmann - Medizinische
Polliklinik der Unviersit Bonn (Bonn, D)
" S. Rickert - Medizinische Polliklinik
der Unviersit Bonn (Bonn, D) " U. Schillings
- Medizinische Polliklinik der Unviersit
Bonn (Bonn, D) " S. Uen - Medizinische
Polliklinik der Unviersit Bonn (Bonn, D)
" R. D・ing - Medizinische Polliklinik
der Unviersit Bonn (Bonn, D) " H. Vetter
- Medizinische Polliklinik der Unviersit
Bonn (Bonn, D) " T. Mengden - Medizinische
Polliklinik der Unviersit Bonn (Bonn, D)
Hypertonie 2005. 29. Wissenschaftlicher Kongress
der Deutschen Hochdruckliga. Berlin, 23.-25.11.2005.
D・seldorf, Kn: German Medical Science;
2006. Doc05hochP109 Die elektronische Version
dieses Artikels ist vollstdig und ist verf・bar
unter: http://www.egms.de/de/meetings/hoch2005/05hoch109.shtml
Ver?ffentlicht: 8. August 2006 ? 2006 Baulmann
et al. Dieser Artikel ist ein Open Access-Artikel
und steht unter den Creative Commons Lizenzbedingungen
(http://creativecommons.org/licenses/by-nc-nd/3.0/deed.de).
Er darf vervielf舁tigt, verbreitet und fentlich
zug舅glich gemacht werden, vorausgesetzt
dass Autor und Quelle genannt werden. ________________________________________
Gliederung " Top " Text Text Einleitung:
Der Augmentations-Index (AIx) quantifiziert
die Pulswellen-Reflexion, ist ein direktes
Ma゚ f・ Gefalter, ein indirektes Ma゚ f・
arterielle Gefsteifigkeit und eng verkn・ft
mit kardiovaskulem Gesamt-Risiko. K・zlich
wurde eine neue Methode entwickelt, welche
aus oszillometrisch am Oberarm aufgezeichneten
Blutdruckkurven den AIx analysiert. Ziel
unserer Studie ist, die herkmliche, als
Goldstandard angesehene, applanationstonometrische
(SphygmoCor) mit der neuen oszillometrischen
Methode, die Augmentation zu bestimmen, (Arteriograph)
zu vergleichen. Material und Methoden: Bei
41 Patienten und Probanden im Alter von 22-74
Jahren wurde jeweils 2 mal tonometrisch mit
SphygmoCor (AtCor Medical, Sydney) sowie
4mal oszillometrisch mit Arteriograph (TensioMed,
Budapest) der AIx bestimmt. Anschlie゚end
wurden die Korrelationen zueinander sowie
zum Alter berechnet. Ergebnisse: Die Korrelation
des AIx von Applanationstonometrie zu oszillometrischer
Methode ist hoch signifikant mit r=0,809
(p<0,0001) und rイ=0,655. Zum Alter waren
beiden Methoden nlich hoch signifikant mit
r=0,76 (SphygmoCor) und r=0,72 (Arteriograph).
Schlussfolgerung: Die oszillometrische Bestimmung
der Augmentation mittels des sehr einfach
anzuwendenden, Untersucher-unabhgigen und
kosteng・stigen Arteriograph birgt ein gro゚es
klinisches Potential zur kardiovaskulen Risikostratifizierung.
|
|
Arterial stiffness The term "arterial
stiffness" once referred only to the
loss of compliance in the large arteries,
now it is a comprehensive term encompassing
the characteristics of the entire arterial
system, including the biochemical-structural-mechanical
changes in the small and large arteries,
as well as the comparative pressures. Cardiovascular
disease is the No. 1 cause of death worldwide.
Heart attack, heart failure and stroke are
the top three within the category. A sudden
jump in blood pressure is the most frequent
cause of stroke, while myocardial infarctions
(heart attacks) are most often caused by
a partial or full coronary occlusion, a rupture
of vulnerable plaque built up during severe
coronary atherosclerosis. In nearly every
case, some stage of the process of sclerosis
is present. In order to prevent severe vascular
crises, it is essential to identify individuals
who are at risk but have not yet developed
symptoms. Identification of at-risk individuals,
examination of the patient for the signs
of preclinical atherosclerosis, as well as
the identification and treatment of the classical
risk factors are included in the European
Guidelines for the management of arterial
hypertension since 2007. "Sudden heart
attack," in the literal sense of the
word, does not exist. The arterial system
prepares for a plaque rupture over the course
of years, or even decades, like a ticking
time bomb. Most severe events can, therefore,
be prevented with early detection of atherosclerosis
(with the help of functional and structural
tests) and preventive treatment begun in
a timely manner. European Guidelines list
the types of target organ damage that can
occur even in asymptomatic patients. The
screening is recommended and mandatory in
every hypertension patient. The Guidelines
emphasize the screening for asymptomatic
atherosclerosis in as large a pool of individuals
as possible, as well as the importance of
such testing for high risk of cardiovascular
disease because together with the traditional
risk factors, it has a greater degree of
predictive value. It is a simple, proven
fact today that arterial stiffness is a truly
important and independent indicator of cardiovascular
risk. The functional and structural changes
in the large arteries are partly age-related,
but there are several conditions that show
a link with accelerated arterial stiffening,
such as hypertension, atherosclerosis, end-stage
renal disease, as well as the traditional
risk factors (diabetes, dyslipidemia, smoking
etc.). That is why arterial stiffness has
become a main topic of clinical research
in recent years, indicated by the huge increase
in publications on the subject. |
| The Scientific World Journal Volume 2013
(2013), Article ID 792693, 6 pages http://dx.doi.org/10.1155/2013/792693
Clinical Study Evaluation of Arterial Stiffness
for Predicting Future Cardiovascular Events
in Patients with ST Segment Elevation and
Non-ST Segment Elevation Myocardial Infarction
Oguz Akkus,1 Durmus Yildiray Sahin,2 Abdi
Bozkurt,3 Kamil Nas,4 Kaz?m Serhan Ozcan,1
Mikl?s Illy?s,5 Ferenc Moln?r,6 Serafettin
Demir,7 M?cahit T?fenk,3 and Esmeray Acarturk3
1Sanliurfa Siverek State Hospital, 63600
Sanliurfa, Turkey 2Department of Cardiology,
Adana Numune Training and Research Hospital,
Adana, Turkey 3Department of Cardiology,
Faculty of Medicine, Cukurova University,
Adana, Turkey 4Department of Radiology, Szent
J?nos Hospital, Budapest, Hungary 5Heart
Institute, Faculty of Medicine, University
of P?cs, P?cs, Hungary 6Department of Hydrodynamic
Systems, Budapest University of Technology
and Economics, Budapest, Hungary 7Department
of Cardiology, Adana State Hospital, Adana,
Turkey Received 18 August 2013; Accepted
15 September 2013 Academic Editors: H. Kitabata
and E. Skalidis Copyright ? 2013 Oguz Akkus
et al. This is an open access article distributed
under the Creative Commons Attribution License,
which permits unrestricted use, distribution,
and reproduction in any medium, provided
the original work is properly cited. Abstract
Background. Arterial stiffness parameters
in patients who experienced MACE after acute
MI have not been studied sufficiently. We
investigated arterial stiffness parameters
in patients with ST segment elevation (STEMI)
and non-ST segment elevation myocardial infarction
(NSTEMI). Methods. Ninety-four patients with
acute MI (45 STEMI and 49 NSTEMI) were included
in the study. Arterial stiffness was assessed
noninvasively by using TensioMed Arteriograph.
Results. Arterial stiffness parameters were
found to be higher in NSTEMI group but did
not achieve statistical significance apart
from pulse pressure . There was no significant
difference at MACE rates between two groups.
Pulse pressure and heart rate were also significantly
higher in MACE observed group. Aortic pulse
wave velocity (PWV), aortic augmentation
index (AI), systolic area index (SAI), heart
rate, and pulse pressure were higher; ejection
fraction, the return time (RT), diastolic
reflex area (DRA), and diastolic area index
(DAI) were significantly lower in patients
with major cardiovascular events. However,
PWV, heart rate, and ejection fraction were
independent indicators at development of
MACE. Conclusions. Parameters of arterial
stiffness and MACE rates were similar in
patients with STEMI and NSTEMI in one year
followup. The independent prognostic indicator
aortic PWV may be an easy and reliable method
for determining the risk of future events
in patients hospitalized with acute MI. 1.
Introduction Acute myocardial infarction
(AMI) continues a worldwide cause of mortality
[1]. In-hospital and 6-month-mortality are
approximately 5-7% versus 12-13%, respectively
[2, 3]. Estimated risk of mortality for AMI
is based on the clinical status of the patients
[4]. Recent studies showed that conventional
risk factors are inadequate for predicting
cardiovascular (CV) mortality and morbidity.
A novel risk factor called arterial stiffness,
which is a defined reduction of the compliance
of arterial wall, and relationship between
coronary heart disease (CHD) have been demonstrated.
Arterial stiffness results in faster reflection
of the forward pulse wave from bifurcation
points in peripheral vessels. As a result
of new waveform, systolic blood pressure
(SBP) increases, diastolic blood pressure
(DBP) decreases, cardiac workload increases,
and coronary perfusion falls down. It plays
a major role in the determination of cardiovascular
outcomes, and it is not inferior to the traditional
risk factors to assess the future risk [5,
6]. Elevated arterial stiffness is associated
with increased major adverse cardiovascular
events (MACE) such as unstable angina, AMI,
coronary revascularization, heart failure,
stroke, and death [7]. Arterial stiffness
parameters including mean arterial pressure
(MAP), pulse pressure (PP), PWV (m/s), and
augmentation index (AI) are directly proportional
to the risk of MACE [8-10]. PWV is a susceptible
diagnostic element, and it is also involved
in risk stratification for subclinical organ
damages [11]. Few studies regarding arterial
stiffness demonstrated that PWV exhibits
a close effect with coronary heart disease
[5, 12, 13]. Whether arterial stiffness parameters
are related to MACE after acute MI has not
been studied sufficiently. The aim of our
study was to compare arterial stiffness parameters
in patients with ST segment elevation (STEMI)
and non-ST segment elevation myocardial infarction
(NSTEMI) and to validate its prognostic value.
2. Patients Ninety-four patients with acute
MI (72 men and 22 women, mean age 60,41 ±
11,17) were included in the study. There
were 45 STEMI and 49 NSTEMI. Data of patients
were analyzed within 24 hours after hospitalization.
All patients received eligible treatment
according to ESC guidelines. The choice of
preparations was entrusted to the investigator.
Hemodynamically compromised patients (Killip
classifications II, III, and IV), patients
with chronic atrial fibrillation and/or flutter,
chronic renal failure, mild-severe valvular
heart diseases and other chronic diseases
were excluded. Our local ethics committee
approved the study, and written informed
consent was obtained from all participants.
Patients were followed up for 12 months.
3. Diagnosis of Acute Myocardial Infarction
Diagnosis of AMI was based on symptoms, elevated
cardiac markers, and electrocardiogram (ECG)
changes. Patients with typical chest pain
plus ECG changes indicative of an AMI (pathologic
Q waves, at least 1?mm ST segment elevation
in any 2 or more contiguous limb leads or
new left bundle branch block, or new persistent
ST segment and T wave changes diagnostic
of a non-Q wave myocardial infarction) or
a plasma level of cardiac troponin-T level
above normal. 4. Laboratory Findings Troponin
T, creatine kinase-MB fraction (CK-MB), serum
urea, creatinine, eGFR, and other hematological
parameters were checked at the admission.
Risk factors, such as hypertension, hyperlipidemia,
diabetes mellitus, cigarette smoking, and
family history, were recorded. Hypertension
was considered as SBP and DBP greater than
140?mmHg and 90?mmHg, respectively, using
an antihypertensive medication. Diabetes
mellitus, hyperlipidemia, and hypertriglyceridemia
were defined as using antidiabetic drugs
or fasting blood glucose over 126?mg/dL,
as plasma low-density lipoprotein cholesterol
(LDL-C) >130?mg/dL, using lipid-lowering
drugs at the time of investigation, and as
TG level >150?mg/dL, respectively, according
to the Third Report of the National Cholesterol
Education Program guidelines. First-degree
relatives who are exposed to coronary artery
disease (CAD) before the age for male is
<55 and female <65 were considered
as family history. 5. Pulse Waveform Analysis
Assessment of arterial stiffness was performed
noninvasively with the commercially available
TensioMed Arteriograph. We collected the
oscillometric pulse waves from the patients.
We measured the distance between the jugulum-symphysis
(which is equal to the distance between the
aortic root and the aortic bifurcation),
and PWV was calculated. Pulse waves were
recorded at suprasystolic pressure. The oscillation
signs were identified from the cuff inflated
at least >35?mmHg above the systolic blood
pressure. In this state there was a complete
brachial artery occlusion, and it functions
as a membrane before the cuff. Pulse waves
hit the membrane, and oscillometric waves
were measured by the device and we could
see the waveforms on the monitor. The AI
was defined as the ratio of the difference
between the second (P2 appearing because
of the reflection of the first pulse wave)
and first systolic peaks (P1 induced by the
heart systole) to pulse pressure (PP), and
it was expressed as a percentage of the ratio
(AI = [P2 ? P1]/PP × 100). SBP, DBP, PP,
and heart rate and other hemodynamic parameters
as return time (RT in sec.), diastolic reflection
area (DRA), systolic area index (SAI %),
and diastolic area index (DAI %) were measured
noninvasively. DRA reflects the quality of
the coronary arterial diastolic filling (SAI
and DAI are the areas of systolic and diastolic
portions under the pulse wave curve of a
complete cardiac cycle, resp.). Hence, the
bigger the DAI and DRA are, the better the
coronary perfusion is. Furthermore, RT is
the PWV time from the aortic root until the
bifurcation and return, so this value is
smaller as the aortic wall is stiffer. |
|
Can arterial stiffness parameters be measured
in the sitting position? Jens N?rnberger,Rene
Michalski,Tobias R T?rk,Anabelle Opazo Saez,Oliver
Witzke,Andreas Kribben DOI: 10.1038/hr.2010.196
Despite the introduction of arterial stiffness
measurements in the European recommendation,
pulse wave velocity (PWV) and augmentation
index (AI) are still not used routinely in
clinical practice. It would be of advantage
if such measurements were done in the sitting
position as is done for blood pressure. The
aim of this study was to evaluate whether
there is a difference in stiffness parameters
in sitting vs. supine position. Arterial
stiffness was measured in 24 healthy volunteers
and 20 patients with cardiovascular disease
using three different devices: SphygmoCor
(Atcor Medical, Sydney, Australia), Arteriograph
(TensioMed, Budapest, Hungary) and Vascular
Explorer (Enverdis, Jena, Germany). Three
measurements were performed in supine position
followed by three measurements in sitting
position. Methods were compared using correlation
and Bland-Altman analysis. There was a significant
correlation between PWV in supine and sitting
position (Arteriograph: P<0.0001, r=0.93;
Vascular Explorer; P<0.0001, r=0.87).
There were significant correlations between
AI sitting and AI supine using Arteriograph
(P<0.0001, r=0.97), Vascular Explorer
(P<0.0001, r=0.98) and SphygmoCor (P<0.0001,
r=0.96). When analyzed by Bland-Altman, PWV
and AI measurements in supine vs. sitting
showed good agreement. There was no significant
difference in PWV obtained with the three
different devices (Arteriograph 7.5±1.6?m?s(-1),
Vascular Explorer 7.3±0.9?m?s(-1), SphygmoCor
7.0±1.8?m?s(-1)). AI was significantly higher
using the Arteriograph (17.6±15.0%) than
Vascular Explorer and SphygmoCor (10.2±15.1%
and 10.3±18.1%, respectively |
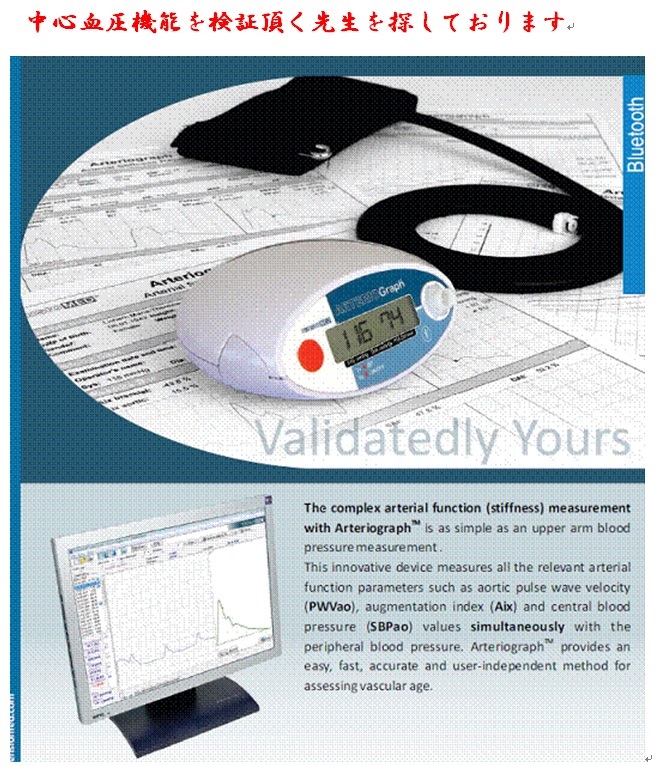
| ALL ABOUT ARTERIES ? - ARTERIOGRAPH Breakthrough
in Early Diagnosis of Arteriosclerosis The
TensioClinic Arteriograph analyses the cardiovascular
system from five highly important aspects
to assure Comprehensive Cardiovascular Risk
Assessment. Measuring Central and Peripheral
Blood Pressure, Arterial Stiffness (PWV &
AIx), Cardiac fitness and considering Classical
Cardiovascular Risk Stratification (Framingham,
SCORE), Arteriograph enables detecting the
real, individual risk even at the early,
reversible stage. Numerous EU references
are available for reinforcing the significance
of this unique screening device, which is
also ideal for evaluating the efficiency
of applied cardiovascular therapy and for
follow up of diabetic patients, too. |
|
Arterial Stiffness Analysis There are various
methods for cardiovascular examination. The
ECG shows signs of oxygen deprivation, when
coronaries are blocked for 70% or more. Other
invasive procedures such as cardiac catheterization
will detect abnormalities at an earlier stage,
but such tests are only performed if people
have complaints. The AORTOGRAM is performed
with the Arteriograph?. This is a relatively
new method that is so sensitive, that abnormalities
can be detected in a very early stage . The
Arteriograph measures both the loss of arterial
functioning and arterial stiffening. Loss
of function is expressed in the unit AIX:
the Augmentation Index. The AIX is a measure
of the total resistance of all blood vessels.
Against this resistance, the heart pumps
every stroke. The higher this resistance
is, the higher the work load for the heart.
An increased resistance of the blood vessels
is caused by loss of function of the endothelium.
Loss of elasticity (stiffness) of the arteries
is expressed in the unit of measure PWV:
Pulse Wave Velocity, or the speed at which
the aortic pulse is going. In case of aortic
stiffening the speed of the pulse increases.
The higher the PWV, the more stiffening of
the aorta has already occurred. Both loss
of function and stiffening are categorized
in four groups: |
| Validation of Arteriograph - A New Oscillometric
Device to Measure Arterial Stiffness in Patients
on Maintenance Hemodialysis Nemcsik J. ?
Egresits J. ? El Hadj Othmane T. ? Fekete
B.C. ? Fodor E. ? Szab? T. ? J?rai Z. ? Jekkel
C. ? Kiss I. ? Tisl?r A. Kidney Blood Press
Res 2009;32:223-229 (DOI: 10.1159/000228935)
Abstract Background: Measuring arterial stiffness
(augmentation index (AI), aortic pulse wave
velocity (PWV)) in hemodialysis (HD) patients
has prognostic significance. To assess its
validity, the new oscillometric Arteriograph
device (AIA, PWVA) was compared to the validated
PulsePen tonometer (AIP, PWVP). Methods:
AI and PWV were measured in 98 patients with
both devices before HD. Validity was evaluated
by Pearson's correlation, Bland-Altman analysis,
and by assessing the prognostic value of
AI and PWV to predict cardiovascular (CV)
mortality over 29 months. Results: Correlation
between AIP and AIA was significant (R =
0.527, p < 0.001). The mean difference
of AI values obtained by the two devices
was -20.6%, and 30% of the paired AI differences
fall outside the ±1 SD boundary of the mean
between-device difference. There was no significant
correlation between the PWVP and PWVA readings
(R = 0.173, p = 0.097). The average difference
of PWV values by the two devices was -1.2
m/s, and 20.6% of the paired PWV differences
fall outside the ±1 SD boundary. In survival
analyses, only PWVP but not PWVA was significantly
related to CV mortality. Conclusion: Lack
of correlation between PWVP and PWVA and
lack of prognostic significance of PWVA suggest
limited validity of Arteriograph to determine
PWV in patients on HD. |
| Smoking and Hypertension Associated With
Greater Arterial Stiffness in People Aging
With HIV By Fred Furtado From TheBodyPRO.com
November 8, 2013 Having HIV is not independently
associated with arterial stiffness -- a trait
linked to cardiovascular disease risk --
despite HIV-infected individuals having a
modest, but clinically significant, increase
in arterial stiffness when compared to their
uninfected counterparts. Instead, factors
such as smoking and hypertension may account
for the increase, according to study results
presented at EACS 2013 in Brussels, Belgium.
To provide some background, HIV infection
has been associated with an increased risk
of cardiovascular disease and one of the
markers for this condition is arterial stiffness,
which is measured by pulse wave velocity
(PWV), or how fast blood moves through the
circulatory system. With age, or other changes
to the arterial wall, blood vessels become
stiffer and blood moves faster through the
system, giving the heart less time to rest.
PWV is directly dependent on mean arterial
pressure (MAP) and past research has shown
that an increase of 1 m/s (meter per second)
in PWV is associated with a 14% greater incidence
in total cardiovascular events. However,
studies measuring PWV in HIV-infected patients
have been small and their results inconsistent.
So, researchers led by Katherine Kooij, M.D.,
compared PWV in a cohort of HIV-infected
and HIV-uninfected people to determine if
there is an independent association between
HIV and PWV, as well as possible determinants
of PWV. Advertisement The study included
566 HIV-infected and 511 HIV-uninfected individuals,
all 45 or older. Both groups had comparable
median ages (52.8 versus 52), gender distribution
(89.1% men versus 86% men) and proportion
of men who have sex with men (76.4% versus
71.4%). However, the HIV-infected group included
more current smokers (32.9% versus 24.8%)
and users of antihypertensive drugs (31.3%
versus 22.4%). The HIV-infected participants
also displayed higher levels of inflammation
and immune activation markers, such as hs-CRP
and sCD163. The researchers performed three
measurements of PWV, as well as systolic
and diastolic blood pressure, using an Arteriograph
system, which registers oscillometric pressure
waves in the aorta through an upper arm cuff.
Additional information on potential determinants
of arterial stiffness was collected with
laboratory measurements and questionnaires.
The data underwent a statistical analysis
with multivariable linear regression models
using PWV as a dependent variable, adjusted
for MAP. The analysis revealed a slightly
higher, but significant unadjusted PWV in
HIV-infected individuals than in HIV-uninfected
individuals (7.9 m/s versus 7.7 m/s, P =
.004). When these results were adjusted for
MAP and gender, the difference between the
two remained at 0.19 m/s (P = .04). If compared
to a PWV increase due to age (+0.29 m/s per
5 years older, P < .001), having a positive
HIV status would be the equivalent of being
3 to 3.5 years older. However, when the PWV
values were adjusted for other factors, such
as smoking and use of antihypertensive drugs,
HIV-infected status was no longer independently
associated with arterial stiffness. In this
setting, the difference between HIV-infected
and HIV-uninfected PWV was only 0.022 m/s
(P = .8). In contrast, every 5 pack-years
(smoking 20 cigarettes a day per year, about
7,305 cigarettes) for current smokers accounted
for a difference of 0.121 m/s (P < .001),
while use of antihypertensive drugs represented
an increase of 0.527 m/s (P < .001). The
researchers also found that the inflammation
marker hs-CRP and the monocyte activation
marker sCD163 were associated with a higher
PWV: 0.039 m/s (P = .001) and 0.056 m/s (P
= .04), respectively. But sCD163 was only
a significant determinant in men.
|
| The Arteriograph is a diagnostic instrument
which is able to measure the severity of
arteriosclerosis. This is the condition of
arterial blockage caused by inflammation
or damage within arteries followed by an
over production of a compound known as plaque
created by the body to repair the damage.
Plaque is made up of cholesterol, minerals
such as calcium, specialised red blood cells
known as platelets and other clotting factors.
The Arteriograph is a simple and painless,
non invasive investigation that can diagnose
arteriosclerosis at an early stage . Symptoms
of arterial blockage include chest pain from
blocking heart arteries, or the loss of sensation,
numbness, or cramp in the lower limbs as
the leg arteries block. These symptoms tend
not to occur until a considerable amount
of an artery is blocked and other arteries
are no longer able to offer effective collateral
circulation. Symptoms of cardiovascular disease
leading to heart attacks and strokes usually
appear only in the last and late stages and
so arterial disease remains unrecognised
through most of its development. The importance
of identifying diseased arteries is clear.
Conventional testing Current investigations
are not designed to detect early occlusion
of blood vessels. The Gold Standard exercise
or stress ECG (where an individual is placed
on a running track with leads on their chest
attached to the ECG), will not necessarily
change until 70% of a coronary (heart) artery
is blocked. More sensitive investigation
such as angiography are invasive and demand
radiation through x-rays and the injection
of a 'dye' to show up the arteries. About
1 in 500 angiographies cause serious or even
fatal events and this figure is even higher
if you take patients who have chest symptoms.
These methods of investigation are effective
only in diagnosing late stage disease and
can carry risks. The results of the Arteriograph
closely correlate to the invasive tests specifically
the Coronary Calcium Score and afore mentioned
Coronary Angiography with the advantage of
avoiding the adverse events. Statistics involving
arterial disease Arteriosclerosis is the
cause of 40% of premature mortality. It is
the main cause of heart attacks and strokes
and can begin at the age of 20 although the
consequences generally appear in our sixth
decade. If we were able to diagnose early
stage disease we would reduce these negative
figures and the Arteriograph, taking only
a few minutes and measuring both small and
large artery resistance (the medical term
for flexibility) is a sensible and valid
method of testing the entire arterial system.
Approximately 48,000 people between the age
of 30-69 have a heart attack each year here
in the UK and 150,000 people suffer a stroke.
The Arteriograph An individual simply has
to avoid food for 3 hours prior to the test
and should not drink alcohol for 10 hours
nor have any caffeine for 6 hours. You shouldn't
be smoking anyway but that should not happen
for at least 3 hours as well! Supplements
and drugs that influence blood pressure should
not be stopped unless authorised by your
GP or prescribing doctor. Most such medication
in most people can be stopped for a few days
without any longer term risk allowing a clear
indication of a patient's arterial status.
After lying down without movement and thinking
nice thoughts for a few minutes then a blood
pressure cuff is inflated around the upper
arm for a few seconds. Other than some tightness
no other discomfort is felt. The specialised
computer inflates the cuff two or three times
as it establishes the measurements and the
nurse will also add in some specific details
including the length from your neck to the
base of your abdomen - the length of your
aorta. The whole process can take as little
as 20 minutess The doctor reading the results
will be able to comment on: " The resistance
(flexibilty) of small arteries " The
resistance (flexibility) of large arteries
" The blood pressure in the aorta -
Central Blood Pressure " Cardiac fitness
" Some other more technical parameters
that may be of use to your doctors The results
are provided to you (and any practitioners
of your choice) with a guide to interpretation.
The benefits of early diagnosis It is very
important to recognise that early diagnosis
of arterial disease allows for intervention
that is capable of slowing down the progress
of arterial disease and at best possibly
reverse the condition. |
| Assessment of arterial stiffness in hypertension:
comparison of oscillometric (Arteriograph),
piezoelectronic (Complior) and tonometric
(SphygmoCor) techniques. Abstract BACKGROUND
Arterial stiffness, measured as aortic pulse
wave velocity (PWV), and wave reflection,
measured as augmentation index (AIx), are
independent predictors for total and cardiovascular
morbidity and mortality. The aim of this
study was to compare a new device, based
on oscillometric pressure curves (Arteriograph),
which simultaneously measures PWV and AIx,
with standard techniques for measuring PWV
(Complior) and AIx (SphygmoCor) in untreated
hypertensive patients. METHODS We compared
PWV and AIx measured using the Arteriograph
with corresponding Complior and SphygmoCor
measurements in 254 untreated hypertensive
patients, age 48 +/- 14 years (mean +/- SD,
range 17-85 years). RESULTS Arteriograph
PWV and AIx were closely related with Complior
(r = 0.60, P < 0.001) and SphygmoCor (r
= 0.89, P < 0.001), respectively. Using
stepwise regression analysis, the independent
determinants of Arteriograph PWV were age,
mean arterial pressure, heart rate and sex
(r(2) = 0.44, P < 0.0001) and for AIx
were age, weight, mean arterial pressure,
heart rate and sex (r(2) = 0.65, P < 0.0001).
The bias between the different techniques
was determined by age and sex for PWV and
age, body weight, sex, heart rate and mean
arterial pressure for AIx. Bland-Altman plots
showed that although the techniques were
closely related, the limits of agreement
were wide. CONCLUSION Although Arteriograph
values and the determinants of PWV and AIx
are in close agreement with corresponding
parameters obtained by Complior and SphygmoCor,
respectively, the techniques are not interchangeable.
|
| The Arteriograph Arteriograph is a new diagnostic
method that can offer reliable and easily
understandible information for the patient
about endothelial function, central blood
pressure and large artery characteristics,
which independently and all together are
significant determinants of cardiovascular
risk. Medical research over the past decade
has provided new possibilities for identifying
early stage arterial stiffening via testing
of large artery compliance. A significant
number of broad, international studies and
conclusions, and international studies designated
as "evidence-based medicine" support
the effectiveness of arterial stiffness related
to cardiovascular disease and its prediction.
Previously these important characteristics
could only be tested under clinical conditions.
As a result of the change in approach in
this area, devices that are easy and safe
to use have appeared, which are able to measure
the parameters that indicate arterial function.
The Arteriograph, developed in Hungary and
patented in over 30 countries, can measure
in a procedure performed on a patient, similarly
to a blood pressure measurement, the biological
characteristics of the condition of the arteries,
which independent of the other well-known
classic risk factors (age, sex, blood pressure,
cholesterol level, smoking habits), reliably
indicates the cardiovascular condition of
an asymptomatic patient and his/her risk
level, and also assists in adjusting existing
blood pressure reduction therapy to an exact
and individualized level. This original,
patented oscillometric method, which has
also been proven invasively, obtains information
from the analysis of the pulse pressure curve
registered in the upper arm. The special,
so-called stop-flow method, i.e. the complete
occlusion of the brachial artery eliminates
the distortion of the pressure curve, so
that the pressure curves are clearly recognizable
and suitable for analysis. The occlusive
measurement period lasts just a few seconds.
The analytic software does not employ a mathematically
generalized transfer function. The determination
of the position and the amplitude of the
reflective wave enable simultaneous and simple
determination of pulse wave velocity, the
augmentation index and the central blood
pressure, as well as complementing the traditional
blood pressure measurement data (systolic,
diastolic blood pressure, arterial medial
pressure, pulse) with further hemodynamic
parameters. |
| Abstracts of the American Society of Hypertension,
Inc. 28th Annual Scientific Meeting and Exposition,
San Francisco, USA May 15-18, 2013 The Journal
of Clinical Hypertension, 2013, Volume 15,
May 2013 Abstract Supplement 28th Annual
Scientific Meeting and Exposition San Francisco,
USA May 15-18, 2013. ________________________________________
Acute Coronary Syndrome Patients: How Stiff
are their Arteries? Deaconu Alexandru Ioan
1 , Tautu Oana Florentina 1 , Fruntelata
Ana Gabriela 2 , Dorobantu Maria 1 1 Emergency
Hospital of Bucharest, Bucharest, Romania;
2 Monza Cardiovascular Center, Bucharest,
Romania Several non-invasive methods are
currently used to assess vascular stiffness.
Pulse wave velocity (PWV) and the augmentation
index (AIx) are the two major non-invasive
methods of assessing arterial stiffness.
A large amount of evidence indicates that
carotid-femoral PWV is an intermediate endpoint
for cardiovascular (CV) events, either fatal
or non-fatal. Central AIx and pulse pressure
have shown an independent predictive value
for CV events in hypertensives and patients
with coronary disease. Studies of arterial
stiffness in patients with cardiovascular
emergencies and acute coronary syndromes,
respectively, are missing. We performed measurements
of arterial stiffness parameters using the
TensioMed Arteriograph in 34 patients admitted
for acute coronary syndromes (ACS), 24 hours
after admission. The study group included
28 males (82.4%) and mean age was 61.7 ±
14.07 years. Arterial stiffness parameters
as aortic PWV, aortic AIx, central systolic
blood pressure (aortic SBP), central pulse
pressure (aortic PP) were analyzed in relation
to clinical, historical and paraclinical
parameters in order to describe particularities
in this patient population. We compared the
results with an age and sex adjusted population
of 34 controls randomly selected from the
most recent Romanian cross-populational statistical
survey, SEPHAR II. In our group, 45.7% of
patients were hypertensive and 37.1% were
diabetic. Most of the patients were on treatment
with ACE inhibitors (91.4%) and beta-blockers
(80%), while 71.1% were on intravenous or
oral nitrates. Mean stiffness parameters
in this group were: aortic AIx=28.51 + 10.81,
with only 14.8% of patients showing normal
values; aortic PWV = 9.71 ± 1.82 m/s; aortic
SBP = 121.71 ± 21.07 mm Hg; aortic PP =
44.39 ± 13.74 mm Hg. No correlations were
identified in this small group between arterial
stiffness parameters and treatment, history
of hypertension or diabetes, type of ACS
and angiographic coronary anatomy. While
aortic AIx was clearly abnormal, reflecting
changes in endothelial function and waves'
reflection, the other parameters of arterial
stiffness were not different from other patient
populations. Aortic AIx is abnormally increased
in patients with acute coronary syndromes.
Parameters of arterial stiffness in patients
with ACS are not related to treatment, type
of coronary disease or previous patient history.
|
|
Invasive Validation of Arteriograph Estimates
of Central Blood Pressure in Patients With
Type 2 Diabetes 1. Niklas Blach Rossen1,2,
2. Esben Laugesen2, 3. Christian Daugaard
Peters3, 4. Eva Ebbeh?j2, 5. S?ren Tang Knudsen2,
6. Per L?gstrup Poulsen2, 7. Hans Erik B?tker4
and 8. Klavs W?rgler Hansen1 + Author Affiliations
1. 1 Department of Medicine, Silkeborg Regional
Hospital, Silkeborg, Denmark; 2. 2 Department
of Endocrinology and Internal Medicine, Aarhus
University Hospital, Aarhus, Denmark; 3.
3 Department of Renal Medicine, Aarhus University
Hospital, Aarhus, Denmark; 4. 4 Department
of Cardiology, Aarhus University Hospital,
Aarhus, Denmark. 1. Correspondence: Niklas
Blach Rossen (niklas.rossen@rm.dk). Received
April 15, 2013. Revision received August
6, 2013. Accepted August 7, 2013. Abstract
BACKGROUND Central blood pressure (BP) has
attracted increasing interest because of
a potential superiority over brachial BP
in predicting cardiovascular morbidity and
mortality. Several devices estimating central
BP noninvasively are now available. The aim
of our study was to determine the validity
of the Arteriograph, a brachial cuff-based,
oscillometric device, in patients with type
2 diabetes. METHODS We measured central BP
invasively and compared it with the Arteriograph-estimated
values in 22 type 2 diabetic patients referred
to elective coronary angiography. RESULTS
The difference (invasively measured BP minus
Arteriograph-estimated BP) in central systolic
BP (SBP) was 4.4±8.7mm Hg (P = 0.03). The
limits of agreement were ±17.1mm Hg. CONCLUSIONS
Compared with invasively measured central
SBP, we found a systematic underestimation
by the Arteriograph. However, the limits
of agreement were similar to the previous
Arteriograph validation study and to the
invasive validation studies of other brachial
cuff-based, oscillometric devices. A limitation
in our study was the large number of patients
(n = 14 of 36) in which the Arteriograph
was unable to analyze the pressure curves.
In a research setting, the Arteriograph seems
applicable in patients with type 2 dia |
|