|
||||||||||||||||||||||
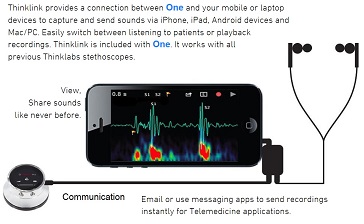
#電子聴診器など色々、#代行輸入します、研究用 |
||||||||||||||||||||||
|
|
||||||||||||||||||||||
#電子聴診器など色々、#代行輸入します、研究用 |
||||||||||||||||||||||
|
|
| #世界初、#着衣の #12誘導心電図電極の決定版 #西陣織り技術と #京都大学の医学で開発された #12誘導心電図に合った ディスポでも、再利用でも可能な、#誰でもが簡単に装着できる心電図電極 #心不全・#心疾患・#狭心症・#不整脈・#心房細動などの #重症疾患に対応、 #遠隔利用が可能で、#在宅・#老人ホーム・#別荘・#ホテル・#旅館・#山荘・#海水浴場 #飛行機・#クルーザ・#船便・#漁船・#ゴルフ・#スポーツ・#農場など幅広い用途に #ほとんど素人でも、#スマホ操作で #12誘導心電図を送信し、#専門医の診断を得られる #帝人フロンティア開発製造・#薬事認可済・#診療報酬適用も症例により可能 |
||||||
|
||||||
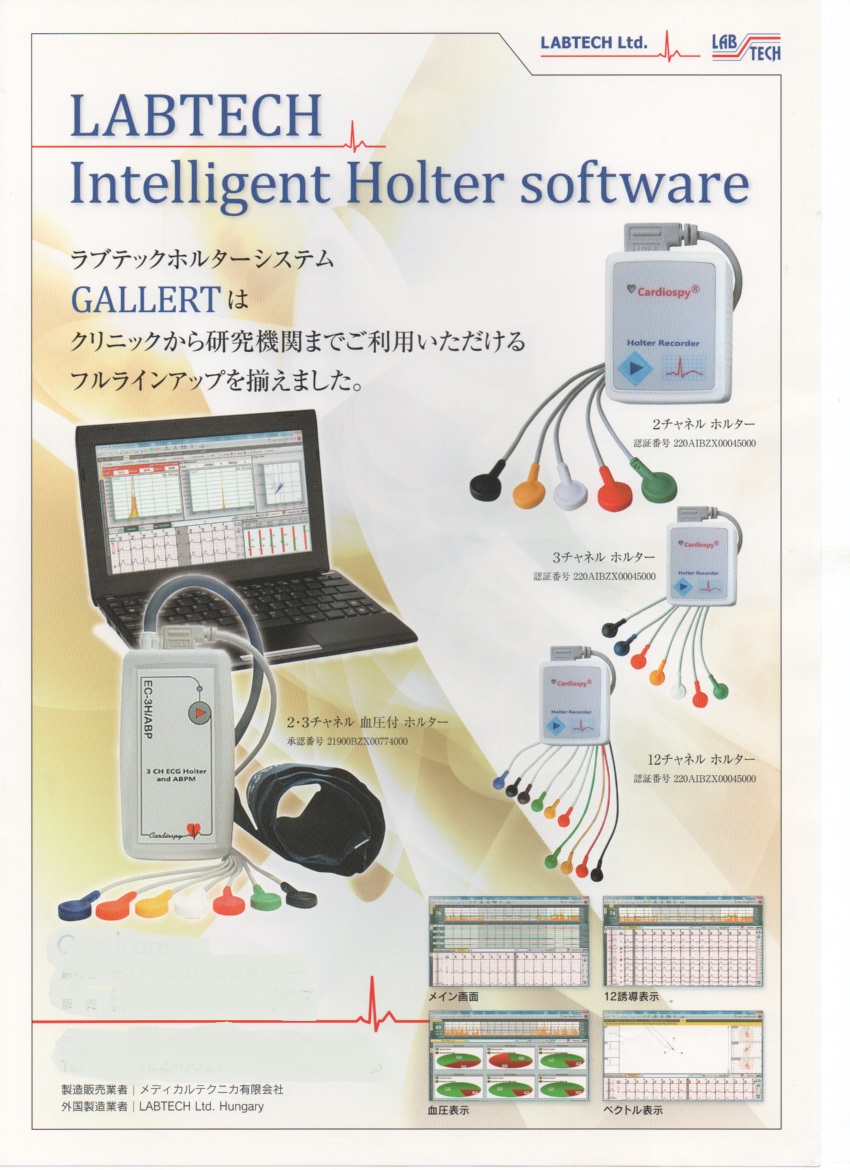
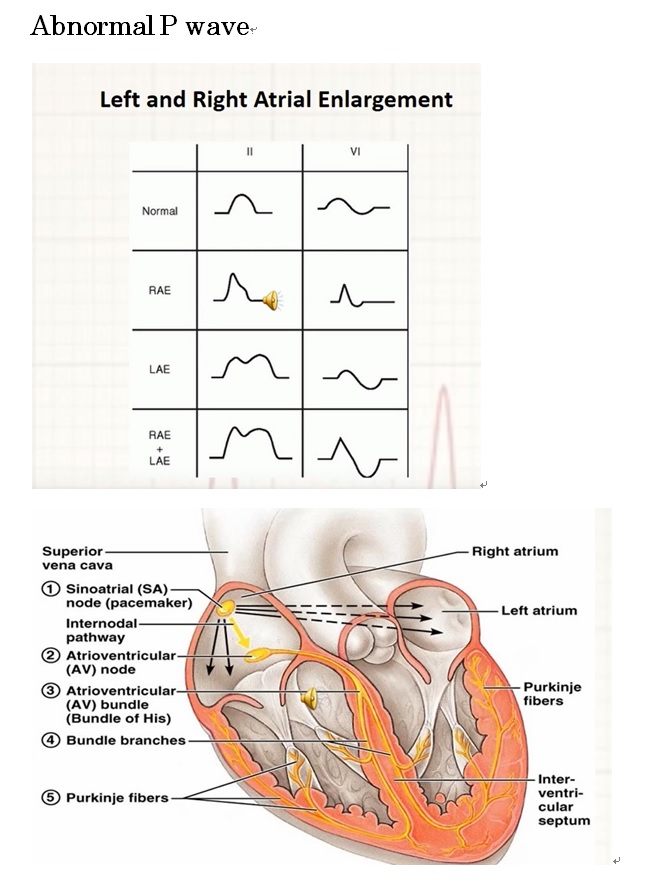
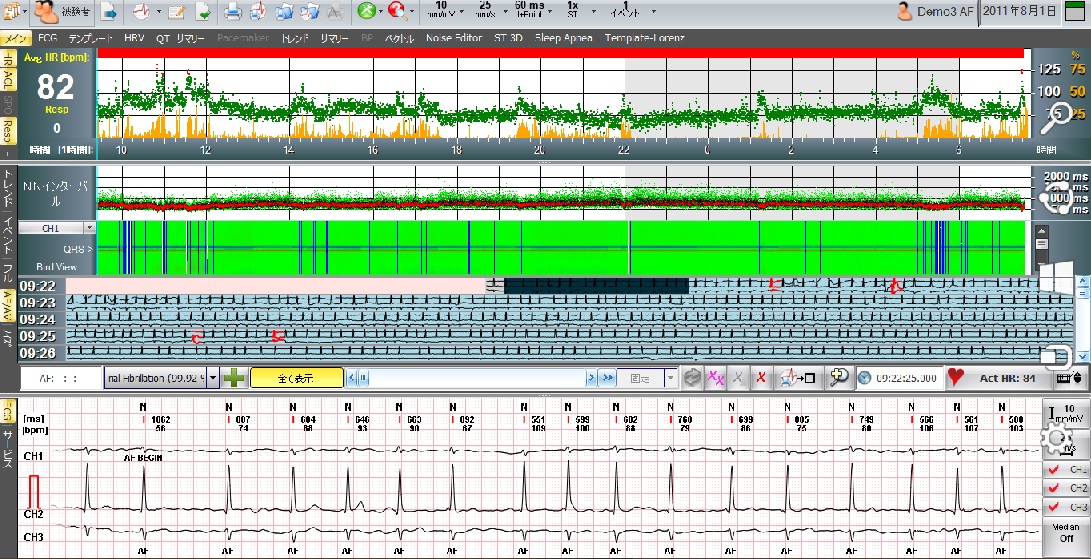
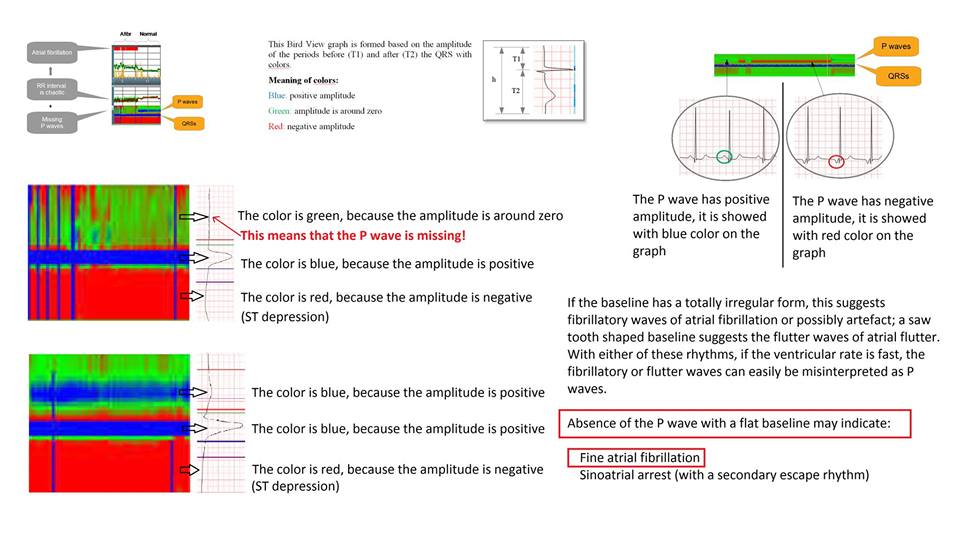
PCの機能が向上し、 #Descrete_Wavelet 手法が、お求めやすい低価格で 実現し、#心房のP波を自動検出できるようになりました、 #心房細動の自動解析能をお試し賜われれば幸いです #臨床用 #薬事認可済 #Labtech社は、当社独自の方法による #P波自動検出と #心房細動自動解析手法 #T_Wave_Alternans #VectorCardiology, #Heart_Rate_Variability , #TWAオルタナンス#Turbulence、#3D可変表示、#Spectral_Analysis等が装備 |
||||||
 |
||||||
|
||||||
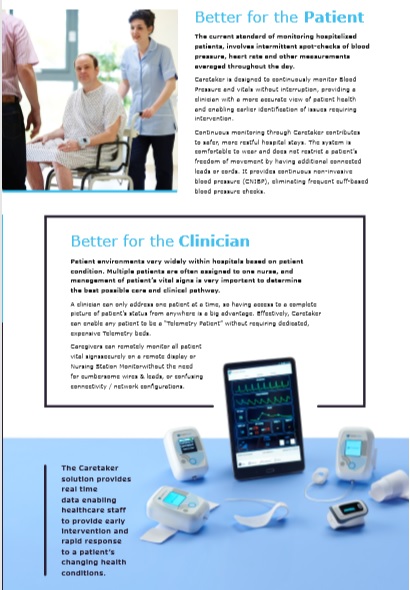
#世界初 #非観血式で連続観血血圧解析手法が #世界麻酔学会にて #2024年検証認証 #ケアテイカメディカル社 #2017年FDA認可 ー #本邦研究用 #メディカルテクニカは、#2007年から本邦導入 #バックアップご用意 #非観血血圧計測で・#連続観血血圧解析・#最先端ディジタル搭載 ・#ポータブル・#ウエアラブル・#一拍毎解析出力付き |
||||||
|
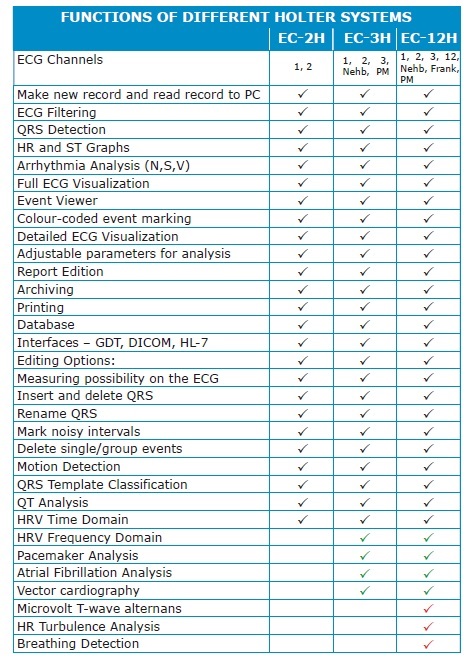
#Cardioview は、#パソコン心電計の #心電図の不整脈解析分類の正確性で、 下記 #検証データが学会で認められています、 #低価格心電計として、#ただ一つ正確さが認められている機種です。 更に、#TeleVital遠隔医療ソフトで #12誘導心電図同時リアルタイム表示可能 |
|||||||||
|
| お問い合わせ先 メディカルテクニカ有限会社 | ||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
| お問い合わせ先 #メディカルテクニカ有限会社 | ||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
|---|---|---|---|
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |